Difference Between In Vivo and In Vitro Fertilization
Starting or growing a family can feel like learning a brand‑new language. When conception doesn’t occur on its own, modern medicine offers two main routes: guiding sperm and egg to meet inside your body (in vivo) or bringing the meeting into the lab (in vitro).
Both paths can lead to pregnancy, but they differ in cost, steps, success rates, and emotional load. We’ll discuss each technique, compare them side by side, break down prices, look at examples, and answer the real questions people type late at night.
What Exactly do “in vivo” and “in vitro” Mean?
They’re location tags which means inside the body versus in the lab.
In vivo translates to “within the living.” When fertilization, testing, or treatment occurs inside a person, animal, or plant, it falls into this category.
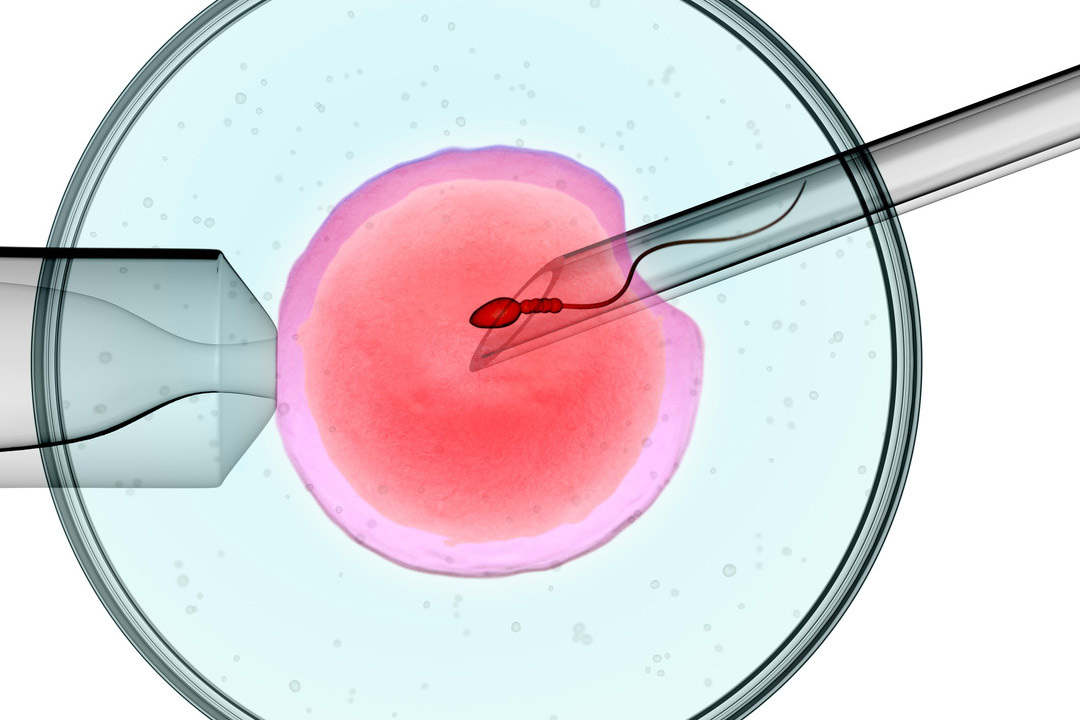
In vitro translates to “in glass.” Eggs and sperm first meet in a dish, test tube, or other controlled setting before the resulting embryo returns to the uterus.
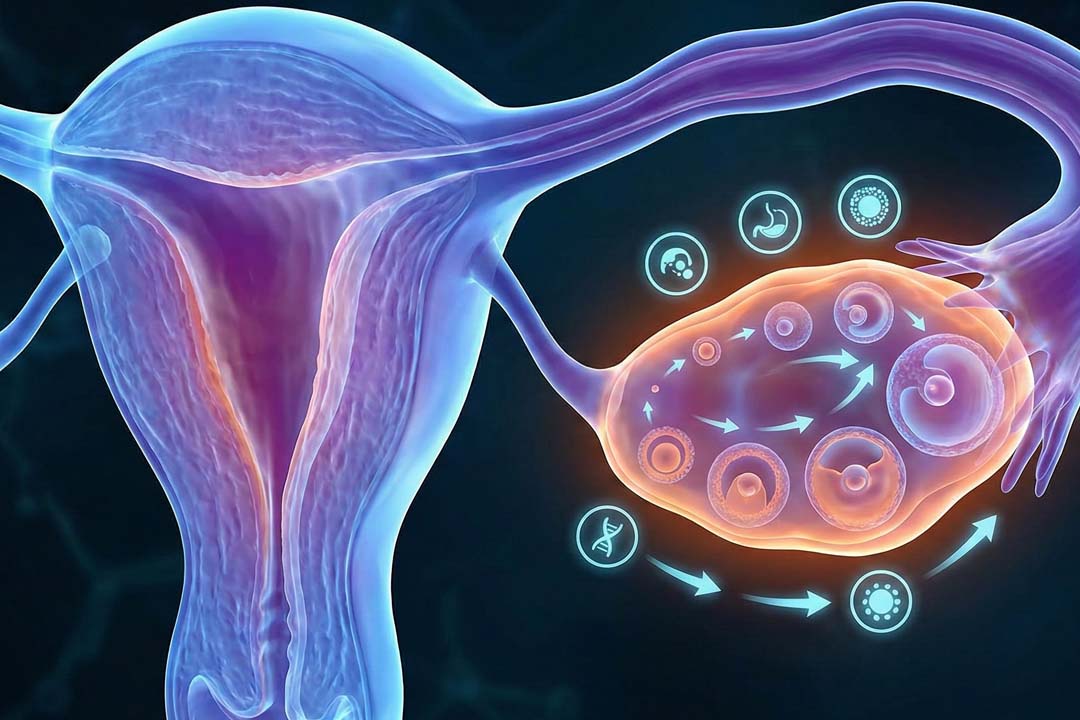
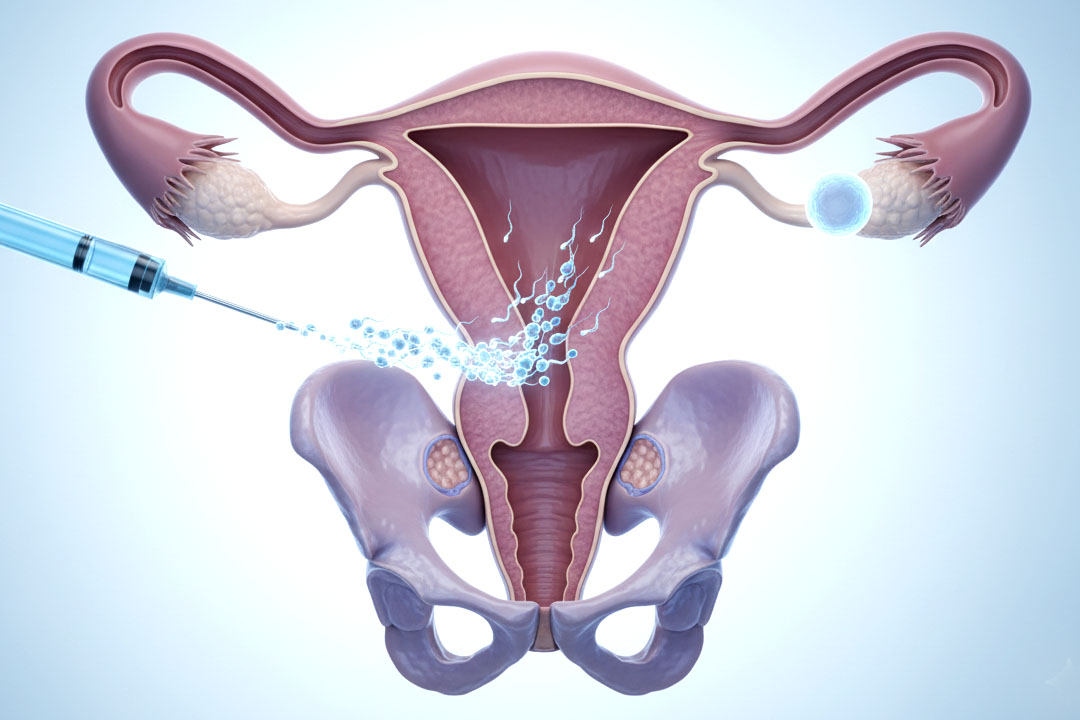
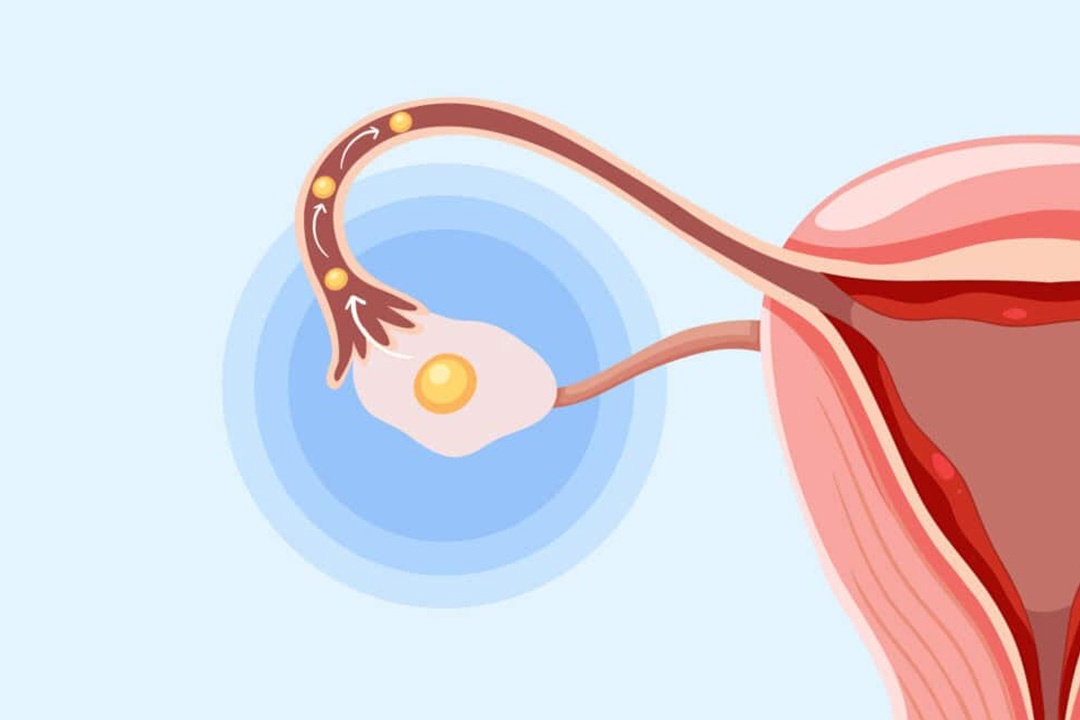
How Does In Vivo Fertilization Work Inside Your Body?
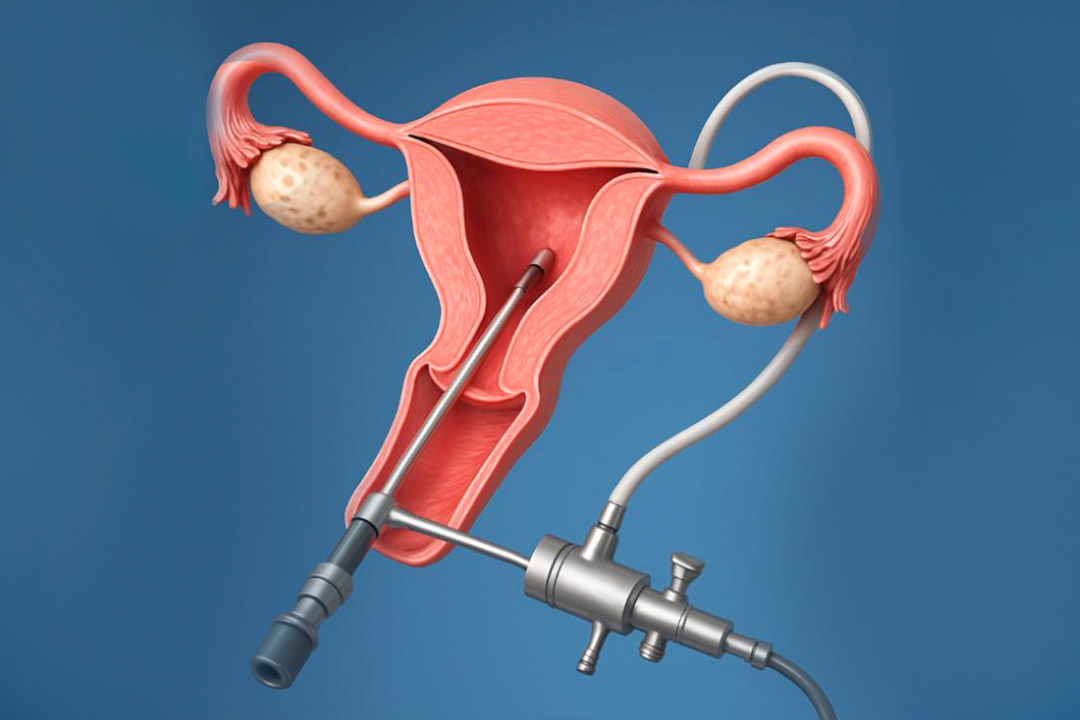
During in vivo procedures, specialists deliver sperm, eggs, or both to the optimal spot, usually the fallopian tube or uterus right when an egg is ready. Fertilization then unfolds in its typical environment, surrounded by hormones, nutrients, and signals only the human body provides.
What Steps are Involved in a Typical In Vivo Cycle?
Most appointments fit into a long morning or afternoon.
- Ovarian priming: You may take mild oral tablets or a short course of hormone injections to encourage one or two eggs to mature.
- Ultrasound tracking: A few painless scans tell the team when the dominant follicle is close to release.
- Sperm wash: Fresh semen is spun in a lab so the most active sperm rise to the top.
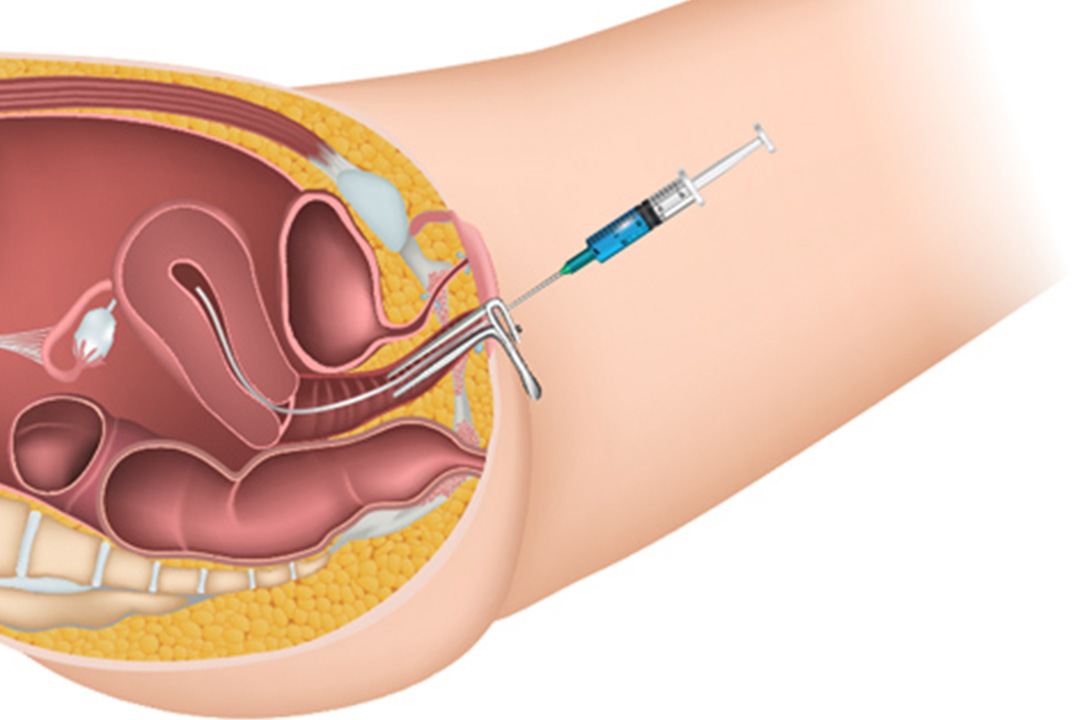
- Careful placement: A thin, flexible catheter introduces sperm (IUI) or both gametes (GIFT) into your uterus or tube.
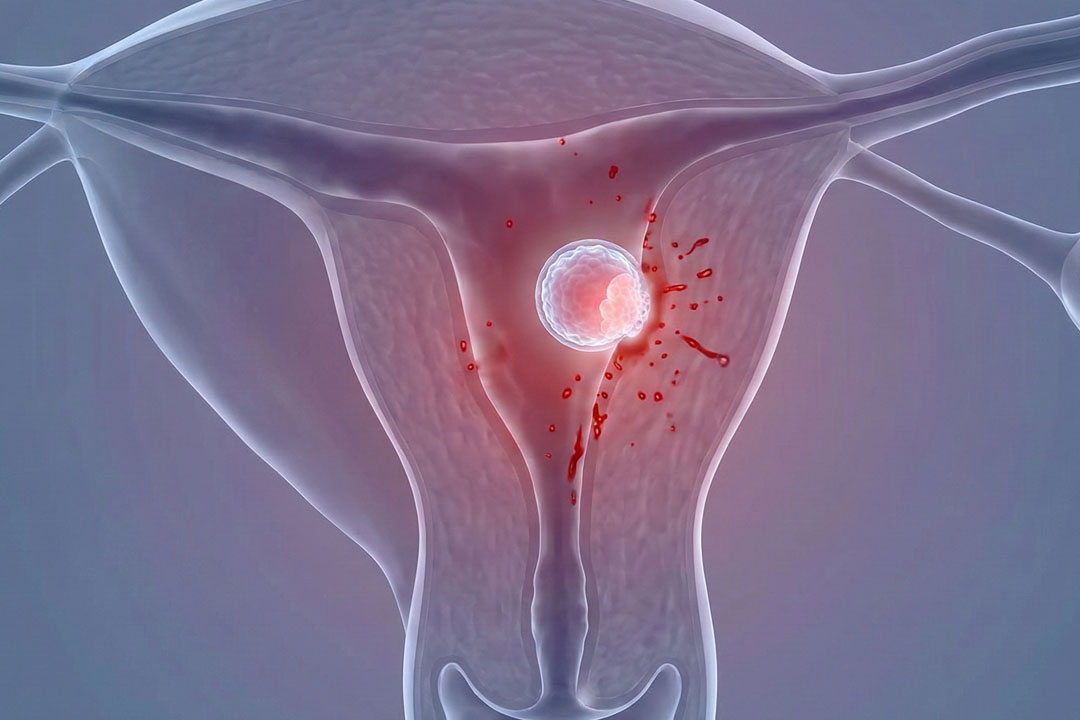
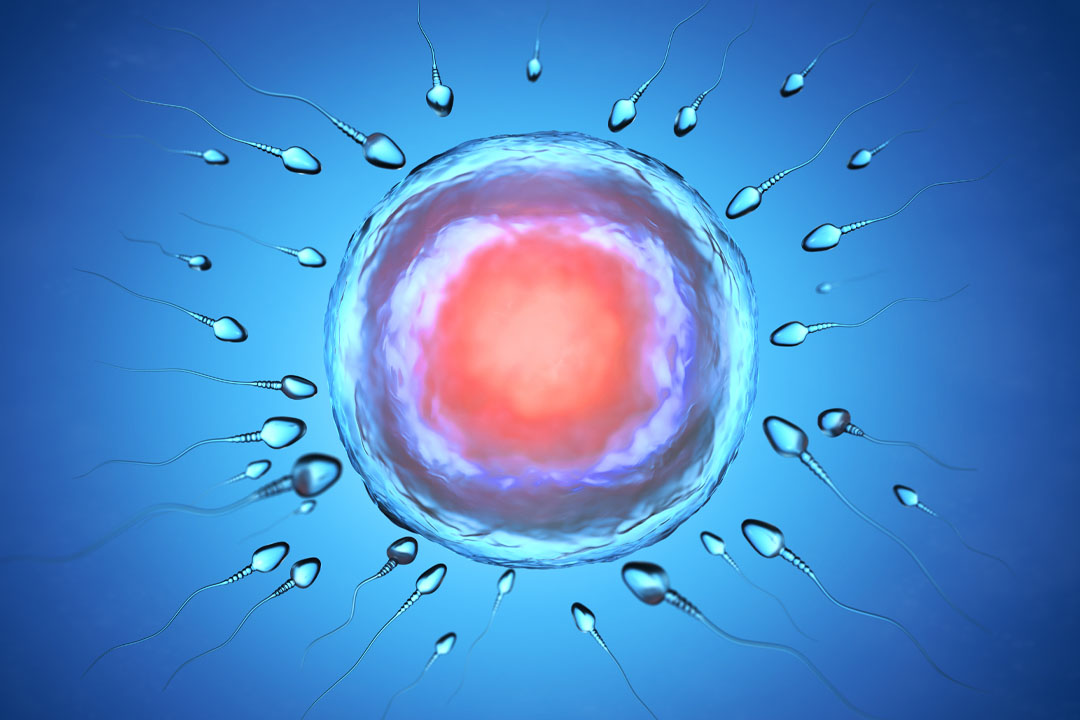
- Natural fertilization: Egg and sperm unite, forming a zygote that travels to the uterus and attempts to implant.
- Pregnancy check: Roughly two weeks later a blood test measures pregnancy hormone levels.
Because most steps use your own cycle’s rhythm, recovery time is short. Many people return to work the same day.
What are the Types of In Vivo Fertilization?
There are three main variations, each filling a different medical niche.
| Method | Definition | Ideal Situations |
|---|
| Intrauterine insemination (IUI) | Washed sperm released directly into the uterus near ovulation. | Mild male‑factor issues, unexplained infertility, single‑parent or donor cases. |
| Gamete intrafallopian transfer (GIFT) | Harvested eggs + washed sperm placed together in the fallopian tube. | Couples with open tubes but years of failed IUIs or unexplained infertility. |
| Zygote intrafallopian transfer (ZIFT) | Eggs fertilized in the lab for a few hours, early zygote moved to the tube. | Tubal factor absent, need to confirm fertilization before transfer. |
All three keep early embryo development inside the body, which some couples find emotionally reassuring.
What is the Cost of In Vivo Fertilization?
Expect lower bills than IVF, with prices affected by region and medication use.
- IUI: Often ₹8,000–₹25,000 per try when using minimal ovulation drugs.
- GIFT/ZIFT: Around ₹75,000–₹1,50,000 because laparoscopy, anesthesia, and lab work add to the bill.
- Extras: Blood tests, ultrasounds, and travel costs mount up, so request an itemized quote.
Some insurance plans cover diagnostic testing but not treatment, so always confirm benefits before you start.
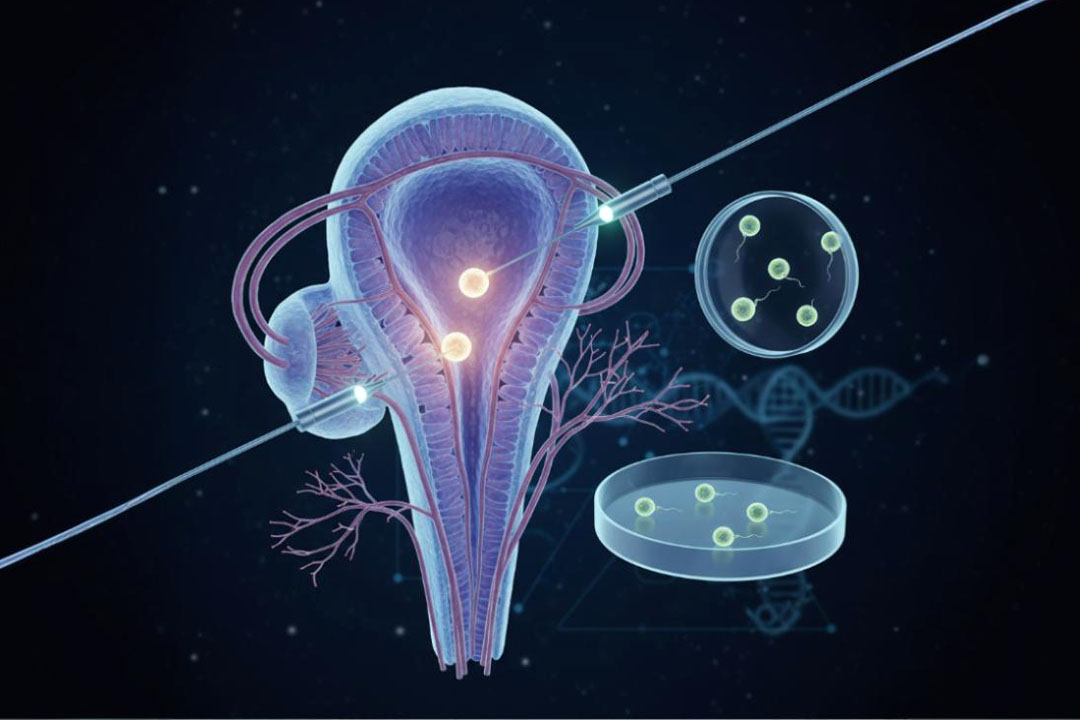
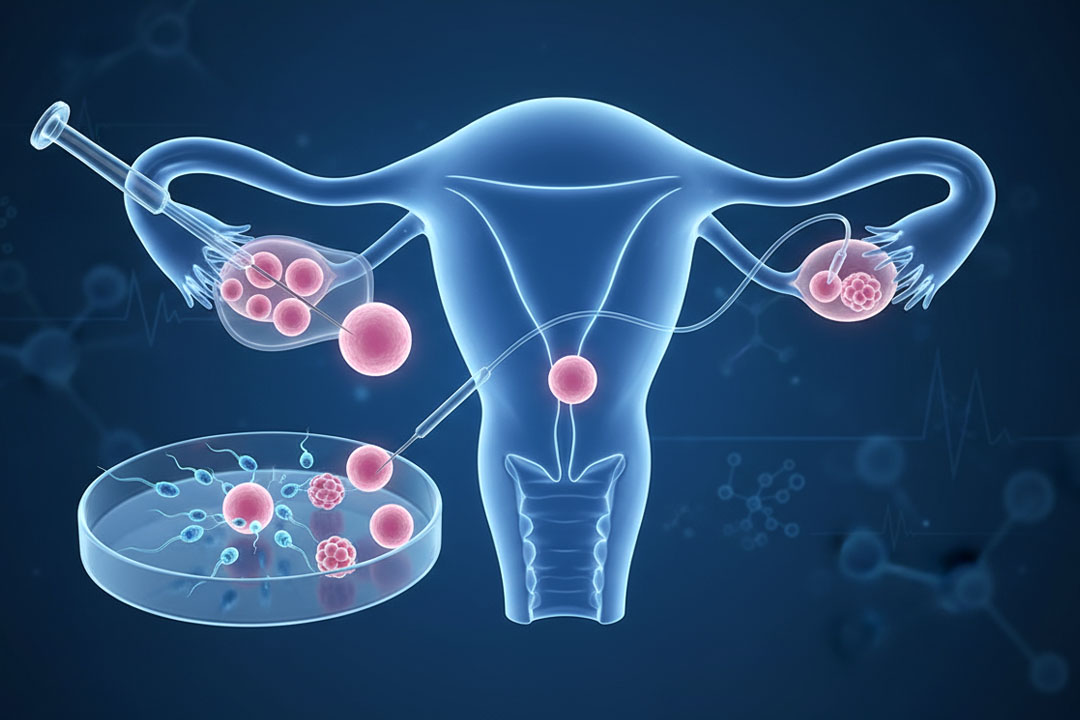
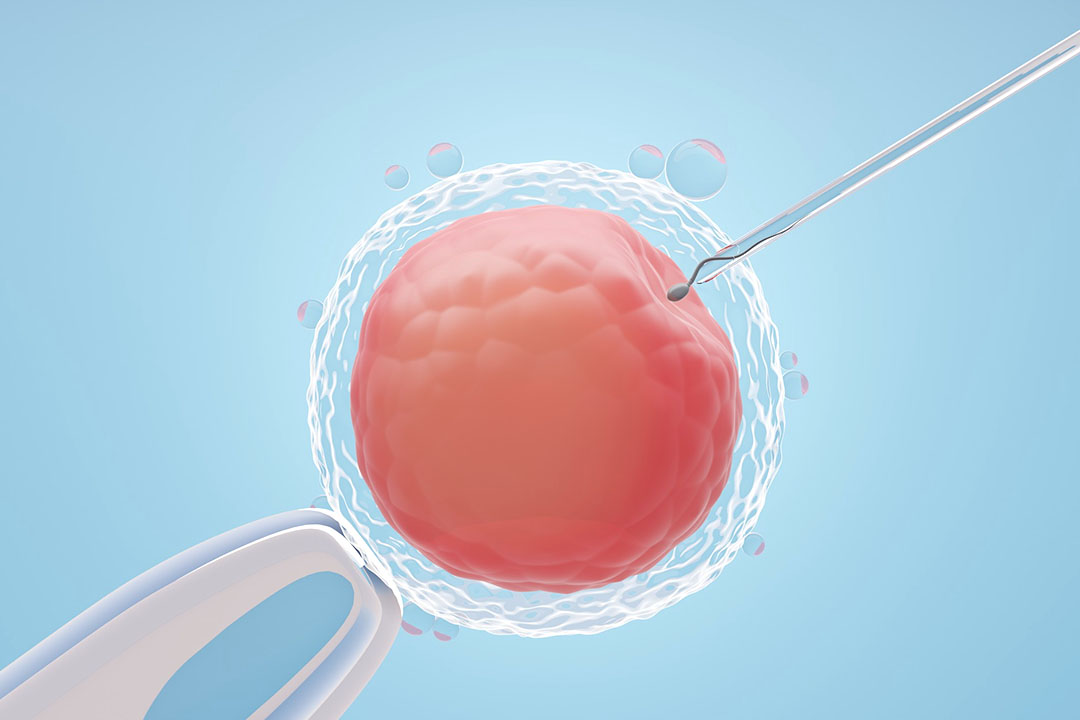
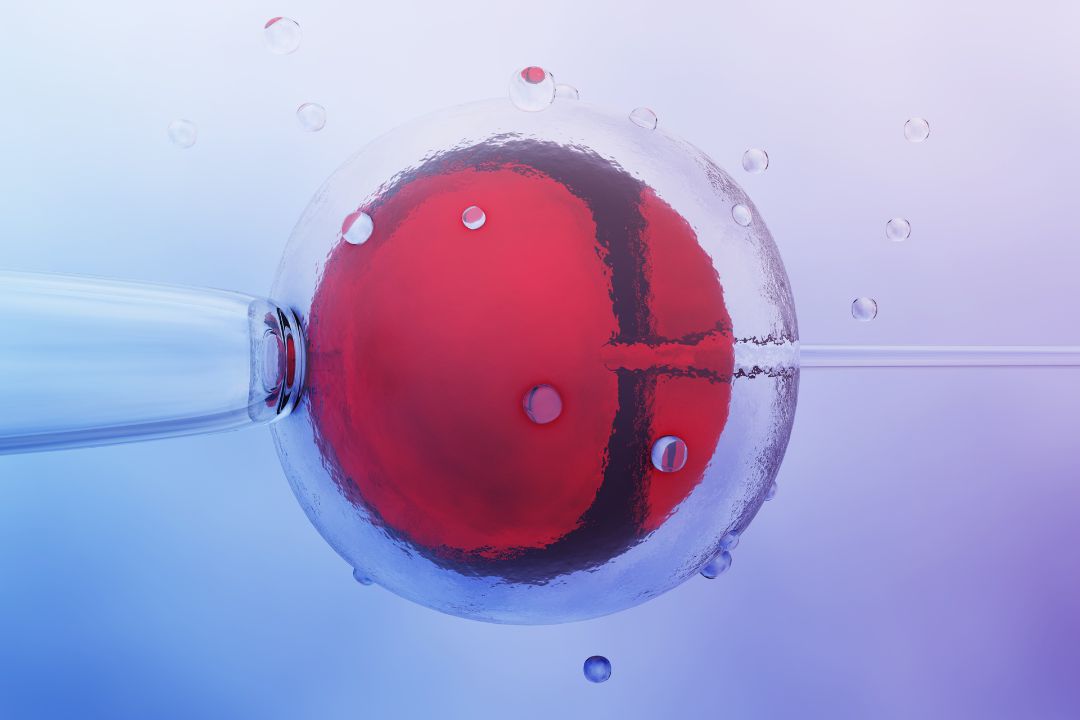
What Happens During In Vitro Fertilization?
In vitro fertilization starts with stronger hormone injections to stimulate many follicles. Eggs are retrieved via a short ultrasound‑guided procedure, combined with prepared sperm, and grown for three to five days. Embryologists grade each embryo, sometimes screen for genetic problems, then prepare your uterus with hormones before transferring one or two embryos.
The timeline usually spans six to eight weeks.
- Suppression or priming: Birth‑control pills or hormone patches fine‑tune your starting hormone levels.
- Stimulation phase: Daily gonadotropin injections for 9–12 days grow multiple follicles.
- Trigger shot: A final hormone injection times egg maturation precisely.
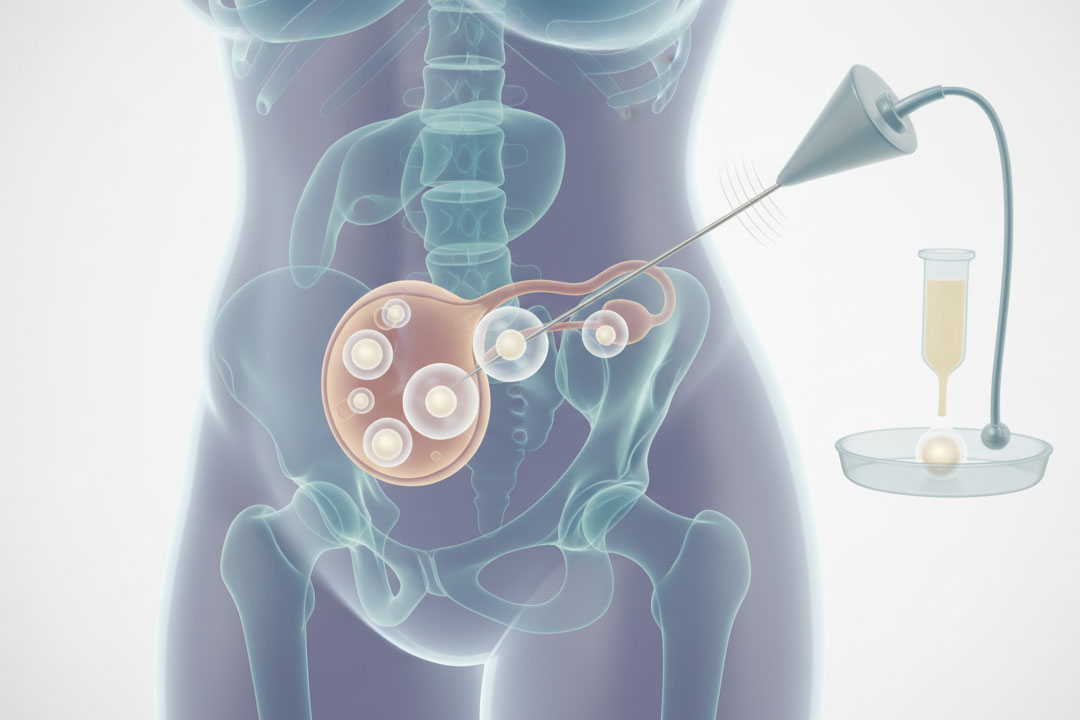
- Egg retrieval: Under light sedation, a thin needle collects eggs through the vaginal wall; you rest for an hour post‑procedure.
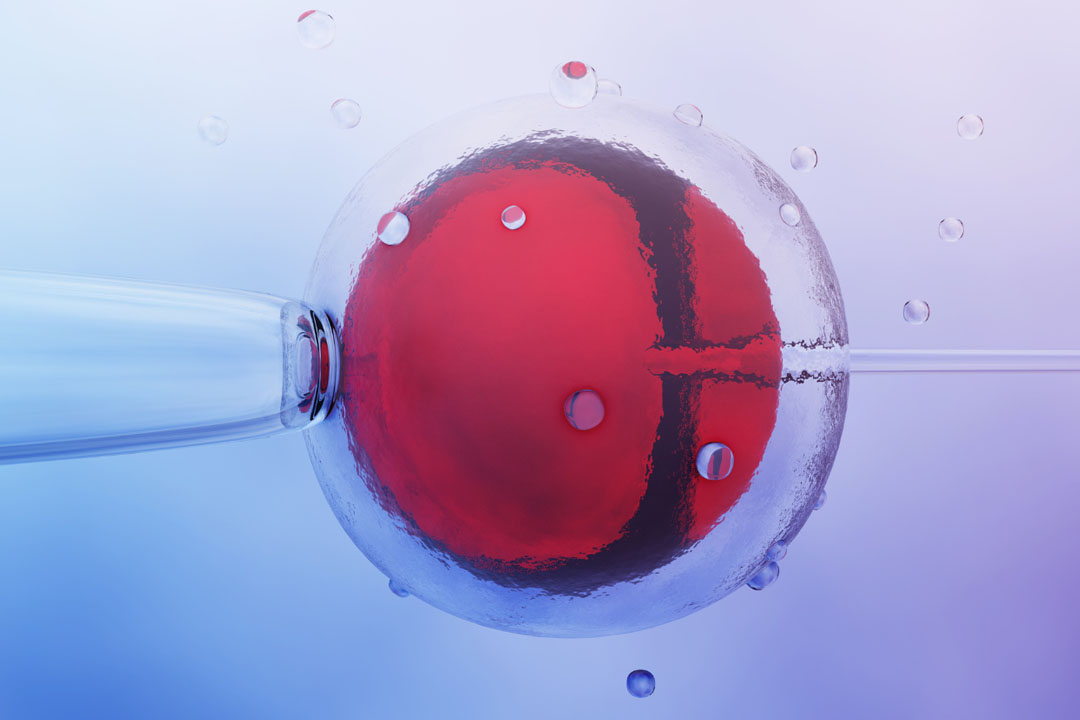
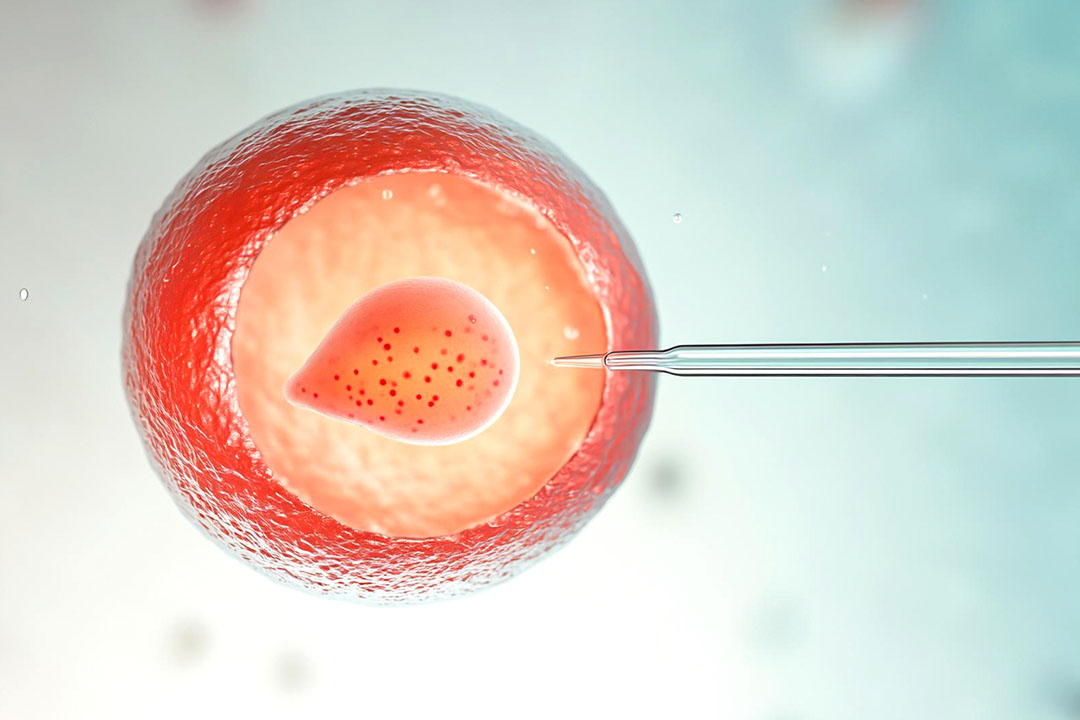
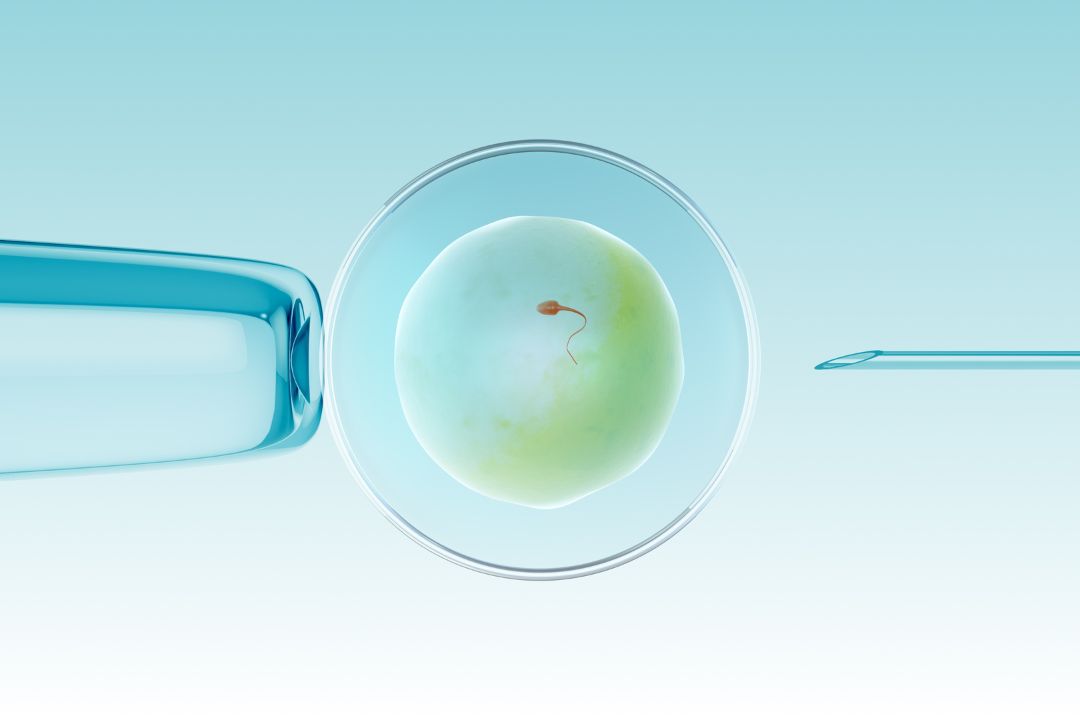
- Fertilization: Eggs meet sperm naturally in a dish or via ICSI (one sperm injected per egg).
- Embryo culture: Lab staff monitor cell division and grade quality.
- PGT option: On day five a few cells can be removed to scan for genetic issues.
- Embryo transfer: A soft catheter places the chosen embryo into your uterus; you’re conscious and home within an hour.
- Two‑week wait: Hormone pills support implantation until the pregnancy blood test.
Frozen embryo transfers use fewer drugs and can be scheduled around work or travel.
Difference Between In Vivo and In Vitro Fertilisation
Location, lab time, cost, and control differ the most.
| Factor | In Vivo Fertilization | In Vitro Fertilization |
|---|
| Location | Inside body (tube or uterus) | Lab dish, then uterus |
| Cycle medication | Minimal to moderate | Moderate to high |
| Lab involvement | Sperm prep only (IUI) or brief egg+sperm handling (GIFT/ZIFT) | Full egg retrieval, culture, possible genetic testing |
| Monitoring | 2–4 ultrasounds and blood draws | 6–10 scans and blood draws |
| Time away from work | Same‑day procedure | Retrieval day off; transfer half‑day |
| Average cost (India) | ₹8k–₹1.5 lakh | ₹1.5 lakh–₹3.5 lakh per cycle |
| Pregnancy rate per try (under 35) | 10–20 % (IUI), 25–30 % (GIFT/ZIFT) | 45–55 % with good embryos |
| Common use cases | Mild male factor, unexplained infertility, early journey | Blocked tubes, severe male factor, failed IUIs, genetic screening needs |
| Risk of multiples | Low (single ovulation) | Higher unless single‑embryo transfer |
What are the Emotional and Lifestyle Considerations?
Your mental well‑being matters as much as your physical health.
- Stress load: IVF involves daily injections and frequent appointments; some people find IUI less demanding.
- Physical recovery: IUI feels like a Pap smear; IVF retrieval can bring a day of bloating and tenderness.
- Support network: Arrange help for injections, clinic rides, or simply an ear when hormones feel overwhelming.
- Work balance: In vivo methods often need fewer schedule changes; IVF sometimes requires flexible leave.
Consider counseling, support groups, or meditation apps to stay grounded along the way.
Are there risks or side effects?
Both routes are safe, but no procedure is risk‑free.
- IUI/GIFT/ZIFT: Mild cramping, light spotting, small risk of infection.
- IVF: Injection site bruises, bloating, ovarian hyper‑stimulation syndrome in 1–5 % of cycles, rare complications from sedation.
- Multiple pregnancy: Higher in IVF when more than one embryo is transferred; can raise chances of preterm birth.
Technological Advancements for In Vivo and In Vitro Fertilization
Technology keeps pushing success rates upward.
- Time‑lapse embryo imaging: Cameras inside incubators capture cell divisions, helping embryologists pick the best embryo without disturbing growth.
- Artificial intelligence grading: Algorithms analyze images for subtle markers of viability, adding another opinion beside human eyes.
- Minimal stimulation IVF: Lower drug doses reduce discomfort and cost, though fewer eggs are collected.
- Cryopreservation upgrades: Vitrification (rapid freezing) boosts survival of frozen embryos, allowing safersingle‑embryo transfers and flexible timing.
- Non‑invasive PGT: Early research suggests embryo DNA can be sampled from culture media, avoiding a biopsy.
These improvements translate into higher live‑birth rates and lower twin rates over time.
Frequently Asked Questions
Does in vivo fertilization hurt?
IUI feels like a Pap smear: mild pressure, brief cramps. GIFT or ZIFT need laparoscopy under anesthesia, so you may be sore for a day.
Can I do IVF if I have blocked tubes?
Yes. IVF bypasses tubes entirely, making it the go‑to option for tubal blockages.
What is the typical gap between IVF cycles?
Most clinics recommend waiting one full menstrual cycle, allowing hormones to return to baseline.
Will ART increase my cancer risk?
Current long‑term studies show no clear link between fertility drugs used in modern doses and higher cancer rates.
Is gender selection possible?
Embryo testing can reveal sex, but many countries restrict selection unless preventing sex‑linked diseases.
How many embryos should I transfer?
Single‑embryo transfer is safest for mother and baby; success rates remain high when the embryo is top‑quality.
Does insurance ever cover IVF?
Coverage is patchy. Some plans cover diagnostic tests but not procedures; others include partial IVF benefits. Check policy fine print.
Can lifestyle changes boost success?
Healthy weight, balanced diet, limited alcohol, no smoking, and stress‑management practices can improve outcomes.
Conclusion
Choosing between in vivo and in vitro fertilization is less about picking a “better” technique and more about matching treatment to your unique situation. In vivo methods, especially IUI offer a gentle, lower‑cost first step when tubes are open and sperm counts only need a head start.
In vitro fertilization provides more control, higher success per cycle, and solutions for blocked tubes, severe male‑factor issues, or genetic concerns. Take time to review medical facts, financial limits, and emotional bandwidth.
Discuss both paths openly with your care team, ask every question you can think of, and remember: plenty of parents have walked these roads before you. Whichever route you travel, a blend of patience, informed choices, and compassionate support will be your compass toward the family you hope to build.
About Us
AKsigen IVF is a premier center for advanced fertility treatments, with renowned fertility experts on our team. Specializing in IVF, ICSI, egg freezing, and other cutting-edge reproductive technologies, AKsigen IVF is committed to helping couples achieve their dream of parenthood. With personalized care and a patient-first approach, AKsigen IVF provides comprehensive fertility solutions under one roof.