Endometrial Receptivity in IVF: Importance, Testing & Success Factors
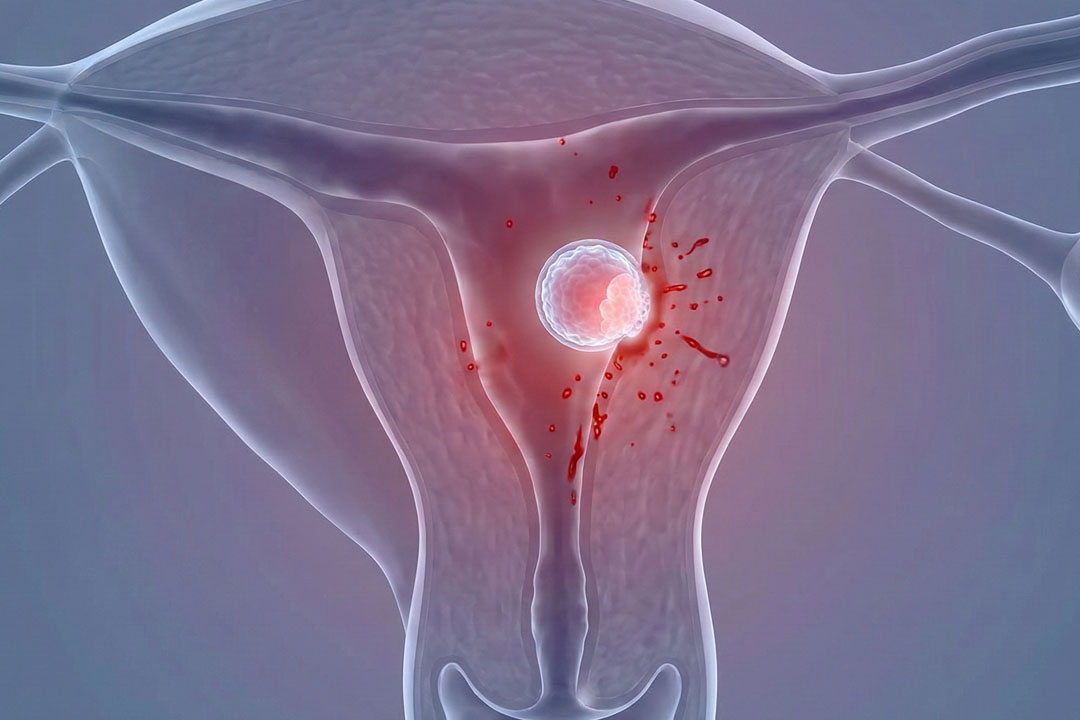
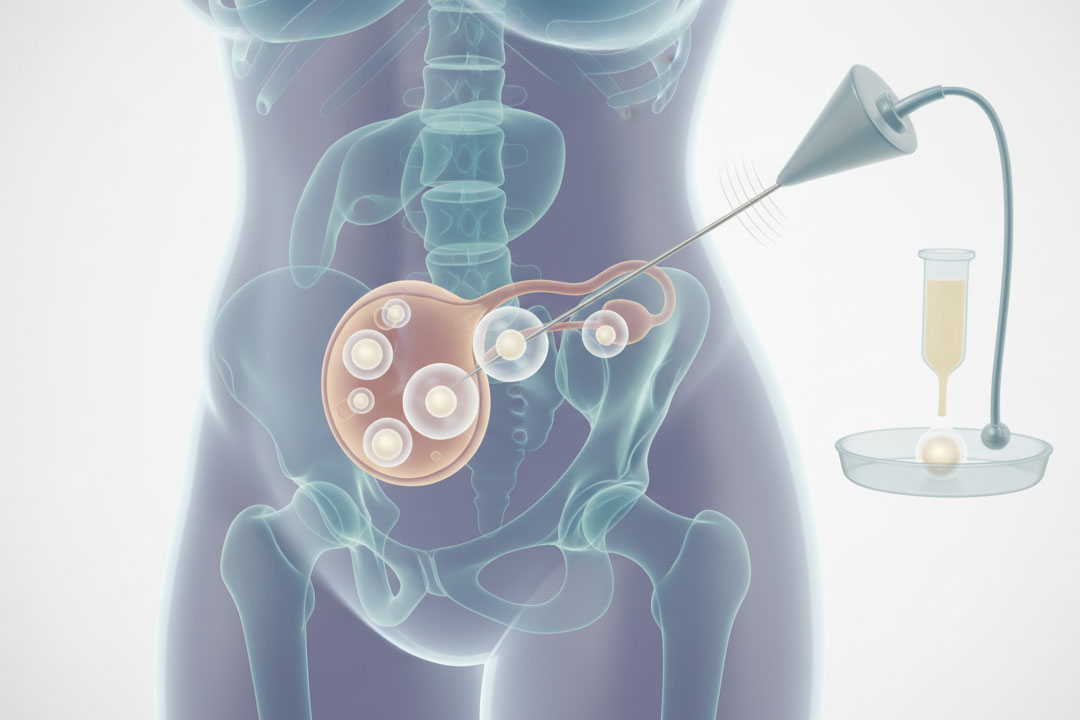
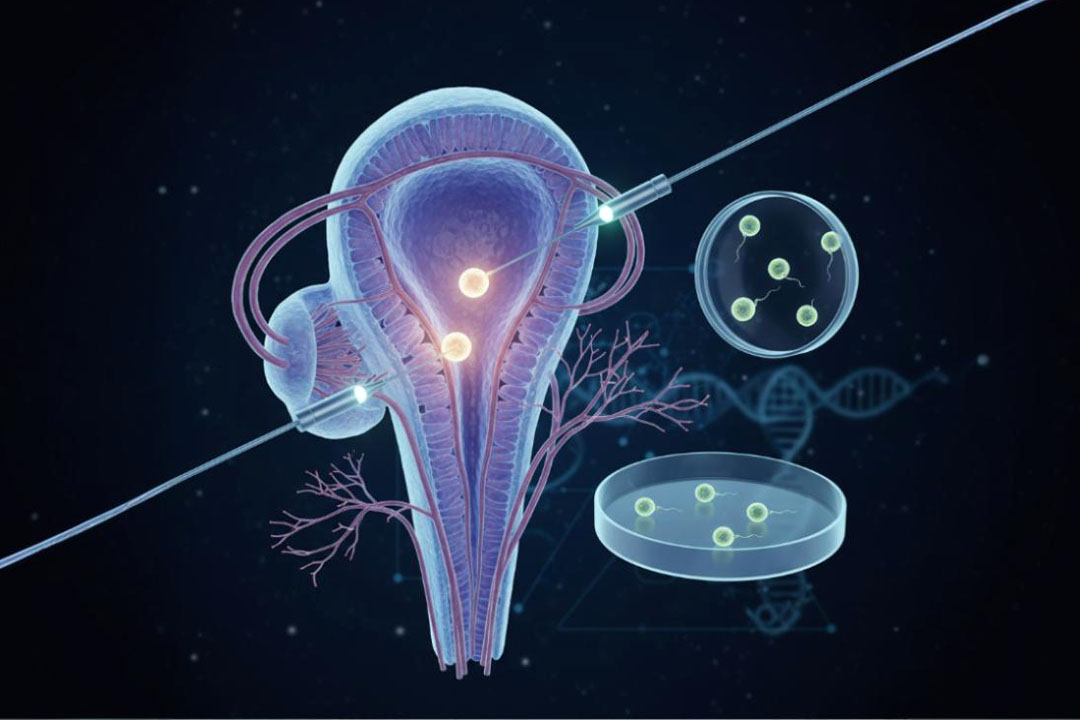
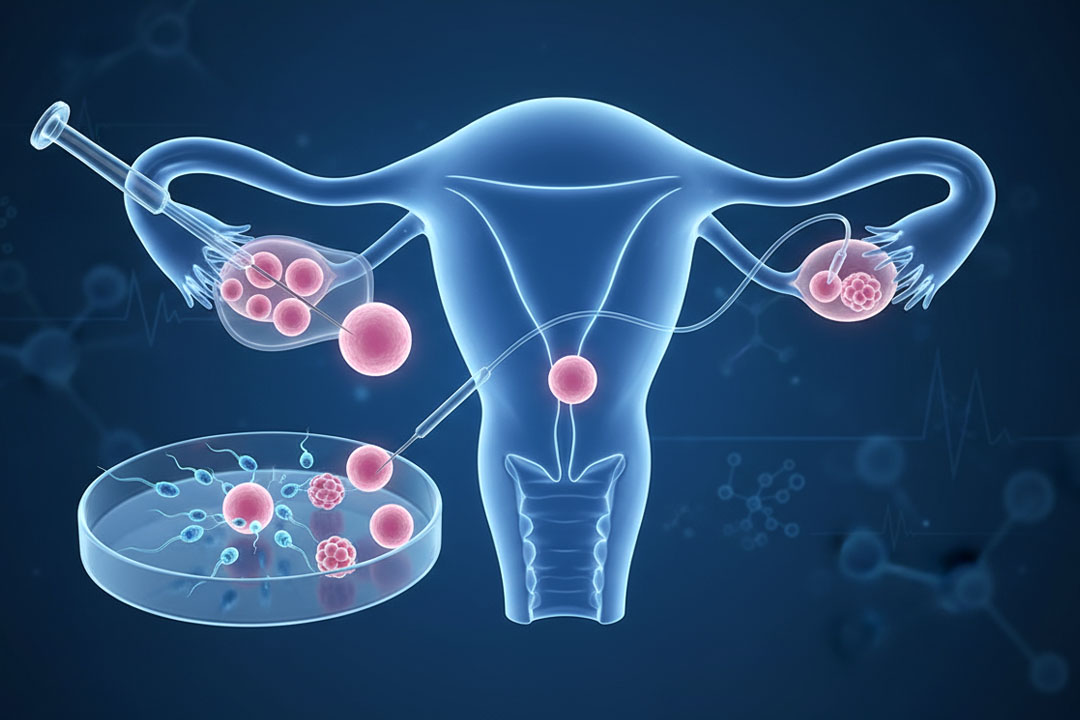
A healthy embryo needs the lining of the uterus, called the endometrium, to get attached. Each cycle, the lining grows under the influence of hormones and then, for a short window, becomes “receptive,” meaning it’s ready for implantation.
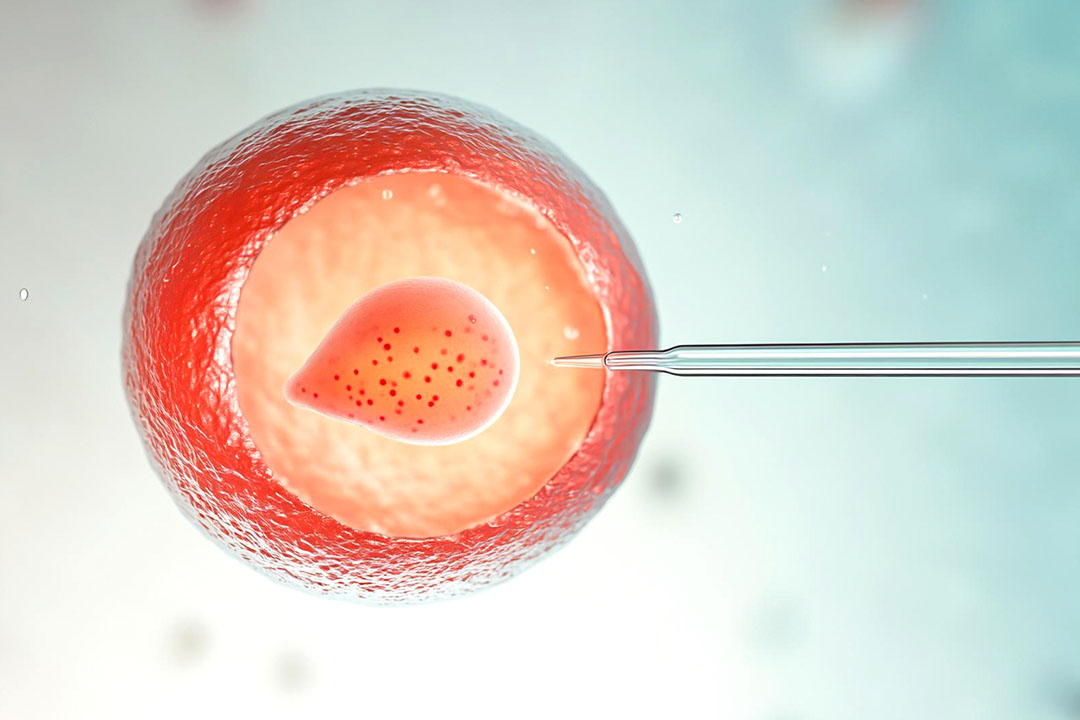
In IVF, doctors try to line up this brief window with the transfer of a good-quality embryo. When timing and lining quality match, the chances of pregnancy improve.
Because many factors can influence receptivity, understanding the basics can help you feel more confident and involved in your care.
What Does “Endometrial Receptivity” Mean?
It’s the short span of often a few days when the uterine lining is ready for an embryo to attach. The endometrium cycles through phases.
Estrogen helps it grow and thicken; then progesterone “matures” it so it can host an embryo. That progesterone-exposed period creates the so-called “window of implantation.”
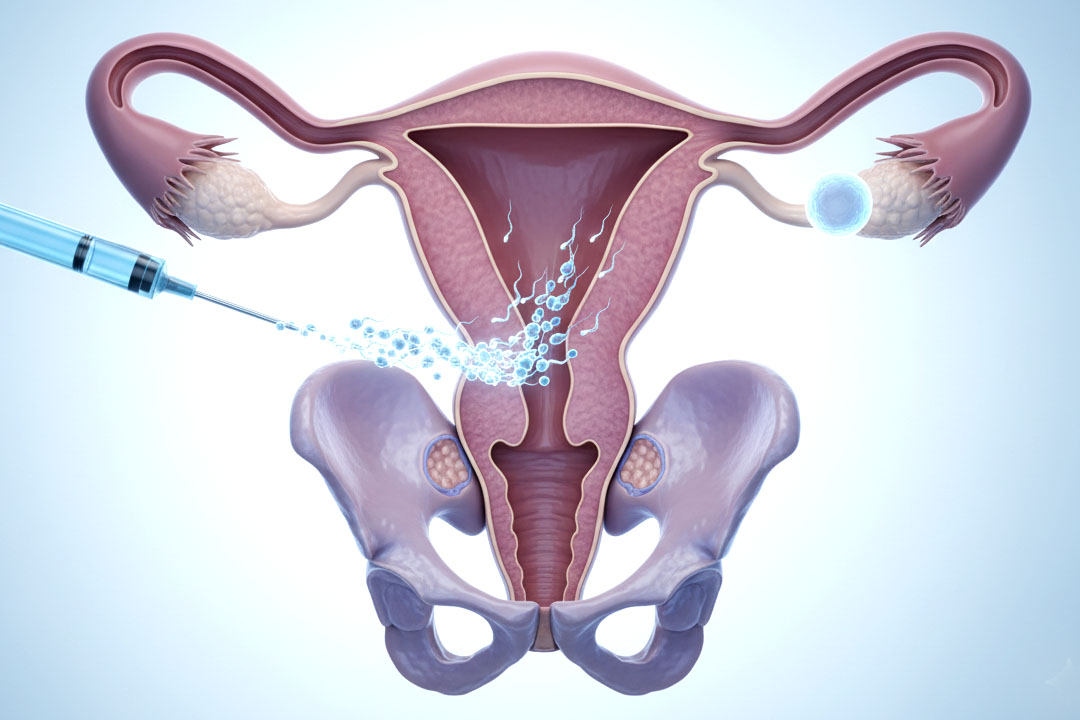
In IVF, clinicians time embryo transfer to coincide with this window, whether you’re in a natural cycle (using your own ovulation), a modified-natural cycle (triggered ovulation), or a fully hormone-prepared (HRT) cycle. The science consistently shows that progesterone exposure is the key switch that opens the window.
How is Receptivity Usually Assessed in Practice?
Doctors rely on ultrasound and clinical context more than exotic tests. Transvaginal ultrasound measures endometrial thickness and looks for a “trilaminar” (triple-line) pattern on the day they plan to start progesterone or perform transfer.
Many programs prefer a thickness around 7–8 mm or more, and a trilaminar look has been associated with higher implantation in some studies. That said, pregnancies can still occur below 7 mm, and thickness alone doesn’t guarantee success, so clinicians consider the full picture.
When is the Transfer Timed in Frozen Cycles?
For blastocyst (day-5/6) embryos, transfer typically occurs after about six days of progesterone exposure (HRT cycles) or roughly six days after the LH surge in true-natural cycles (or ~7 days after an hCG trigger in modified-natural cycles).
These schedules reflect the way progesterone matures the lining to match a day-5/6 embryo. Small adjustments may be made based on your protocol and embryo day. Evidence supports these broad timing rules, while acknowledging individual variation.
Why does Progesterone Matter?
Progesterone turns a growing lining into an accepting one. Estrogen builds the lining bujt progesterone changes its structure and gene activity to enable implantation. In HRT-FET cycles, clinics carefully control when progesterone starts, because that start time “starts the clock” for the window.
Research continues on whether measuring serum progesterone and adjusting the dose on or before transfer helps; emerging data suggest add-on dosing can be considered when levels are low, but practices vary.
What Uterine Issues Can Reduce Receptivity?
Common, fixable problems include polyps, submucosal fibroids, adhesions, and infections like chronic endometritis.
Small intrauterine growths or scar tissue can distort the lining, and treating them (often via hysteroscopy) may improve the environment. Chronic endometritis (a low-grade inflammation of the lining) is increasingly recognized.
Some studies in people with repeated implantation failure show better outcomes after antibiotics when a follow-up biopsy confirms cure, though other research finds mixed results. Your team may test and treat based on your history and findings.
Blood Flow Scans, Scratch, PRP and Other Add-ons
Doppler measures of blood flow and “endometrial scratch,” once popular, haven’t consistently improved live-births across large, well-designed studies. PRP (platelet-rich plasma) and other adjuvants are being explored in specific situations but remain investigational for most patients.
It’s reasonable to ask your doctor whether a proposed add-on has strong, randomized-trial evidence for someone with your history. (Guidelines on embryo transfer emphasize focusing on fundamentals: a well-timed transfer of a good embryo into a healthy cavity.)
Building a Receptive Lining
Endometrial receptivity is complex in nature and thus it is important to follow the guidelines given by your doctor, but the general idea consists of:
1) Choose the right cycle type for you
Options include true-natural, modified-natural, and HRT (programmed) frozen-embryo cycles. Natural approaches rely on your own ovulation; HRT cycles use prescribed estrogen and progesterone to control timing precisely. The choice depends on your cycle regularity, medical history, and clinic logistics.
2) Get the timing of progesterone right
Your team will plan embryo transfer after a specific number of progesterone days to match embryo age (e.g., blastocyst = P+6 in HRT cycles). Keep medication schedules exact; a missed or late dose can shift the window.
3) Optimize the uterine cavity
Before transfer, many clinics screen for polyps, fibroids that indent the cavity, adhesions, or chronic endometritis and address them if found. This can be as simple as an ultrasound and cavity evaluation, with hysteroscopy if needed.
4) Mind the basics
Healthy sleep, stress management, stopping tobacco, and managing conditions like thyroid disease or diabetes support overall fertility care. While lifestyle steps can’t “force” receptivity, they contribute to overall treatment readiness.
Frequently Asked Questions
How much does IVF cost in India (roughly)?
Prices vary by city and inclusions, but a single IVF cycle commonly ranges ₹1,20,000–₹2,50,000, with additional costs for medicines, ICSI, freezing, or genetic testing if used. Always ask for a written breakup of costs for your exact plan.
What is “thin endometrium,” and should I cancel IVF if mine is thin?
“Thin” usually refers to <7 mm on ultrasound, but this is a guide and not a rule. Some people conceive below this number. Your team may try extra estrogen time, different routes (oral/patch/injectable), or consider adjuvant options, then decide whether to proceed or adjust the cycle.
How long should I be on progesterone before transfer?
For a warmed blastocyst in an HRT cycle, many clinics aim for about six full days of progesterone before transfer; natural or modified-natural cycles align transfer with LH+6 or hCG+7. Your clinic may tweak this based on embryo day and your schedule. Take medications exactly as instructed.
Do blood tests for progesterone on transfer day matter?
Some clinics check a serum progesterone around transfer; if it’s low, they may add or adjust dosing. Research is evolving, and practices vary. Ask your team whether they monitor levels and how they act on the results.
What to do if I have chronic endometritis (CE)?
Your doctor may suggest an endometrial biopsy with special staining. If CE is confirmed, antibiotics are usually prescribed and a follow-up test may be done to confirm it’s cleared before trying again. Evidence suggests outcomes are better when cure is documented, though not all studies agree.
Do transfer skills and lab quality matter as much as receptivity?
Yes. A careful transfer technique and a well-equipped lab are crucial. Professional societies publish guidance on optimizing the transfer itself, emphasizing fundamentals alongside any add-ons.
Can lifestyle improve receptivity?
Lifestyle can’t replace medical steps, but good sleep, stopping tobacco, moderating alcohol, and managing conditions like thyroid disease support your overall fertility plan. Think of it as making everything else work a bit better.
Conclusion
Endometrial receptivity is about getting the timing and the environment right. When progesterone exposure matches the embryo’s age, and the uterine cavity is healthy and well-prepared, the odds of implantation improve. Ultrasound thickness and a trilaminar pattern are helpful guides, but they aren’t the whole story as many factors work together, from embryo quality and transfer technique to treating issues like polyps or chronic endometritis.
Most people won’t need specialized add-on tests; a careful, stepwise plan usually serves best. If cycles haven’t worked before, review the basics with your care team: confirm the cavity is normal, check for inflammation, align progesterone timing precisely, and consider embryo-related factors.
About Us
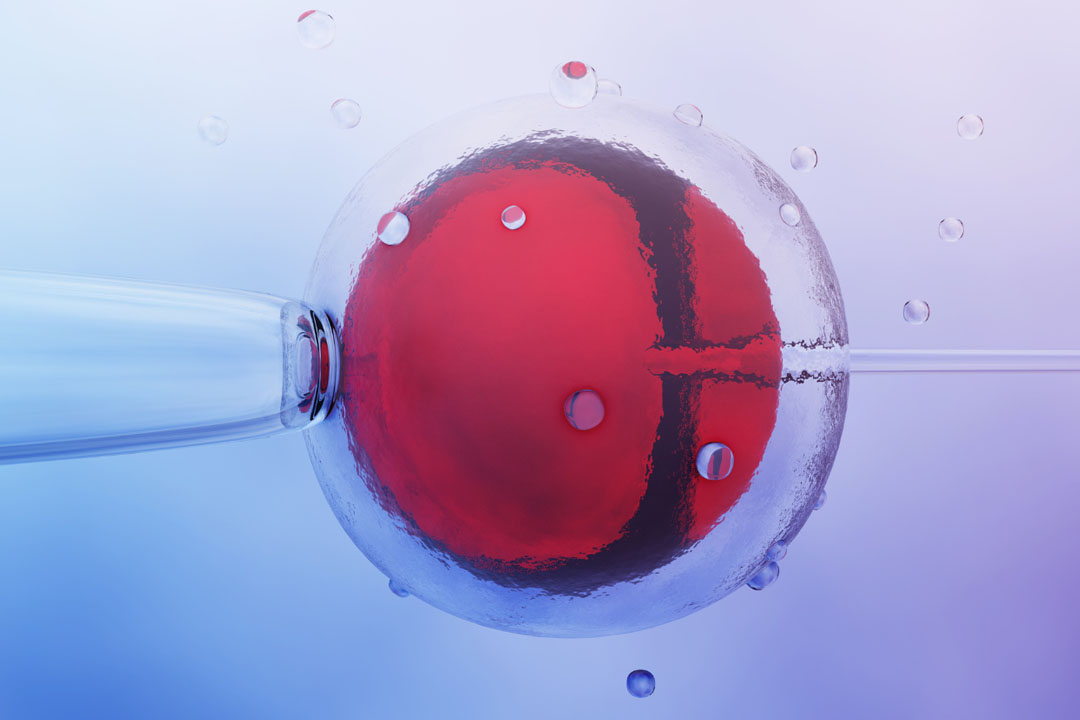
AKsigen IVF is a premier center for advanced fertility treatments, with renowned fertility experts on our team. Specializing in IVF, ICSI, egg freezing, and other cutting-edge reproductive technologies, AKsigen IVF is committed to helping couples achieve their dream of parenthood. With personalized care and a patient-first approach, AKsigen IVF provides comprehensive fertility solutions under one roof.