Hysteroscopy Procedure Step by Step
Hysteroscopy is a minimally invasive way to examine the uterus and, when needed, treat small problems without an abdominal cut. It uses a thin, lighted tube called a hysteroscope, passed gently through the vagina and cervix.
For many people, this single procedure can both explain symptoms like heavy or irregular bleeding and fix the cause in the same sitting.
Recovery is usually faster than open surgery because there are no external incisions, and most people go home the same day.
If your periods are unpredictable, if you’ve had spotting between cycles, or if scans suggest growths like polyps or fibroids, your clinician may recommend hysteroscopy to get a clear view and, if necessary, remove the problem safely.
What is Hysteroscopy?
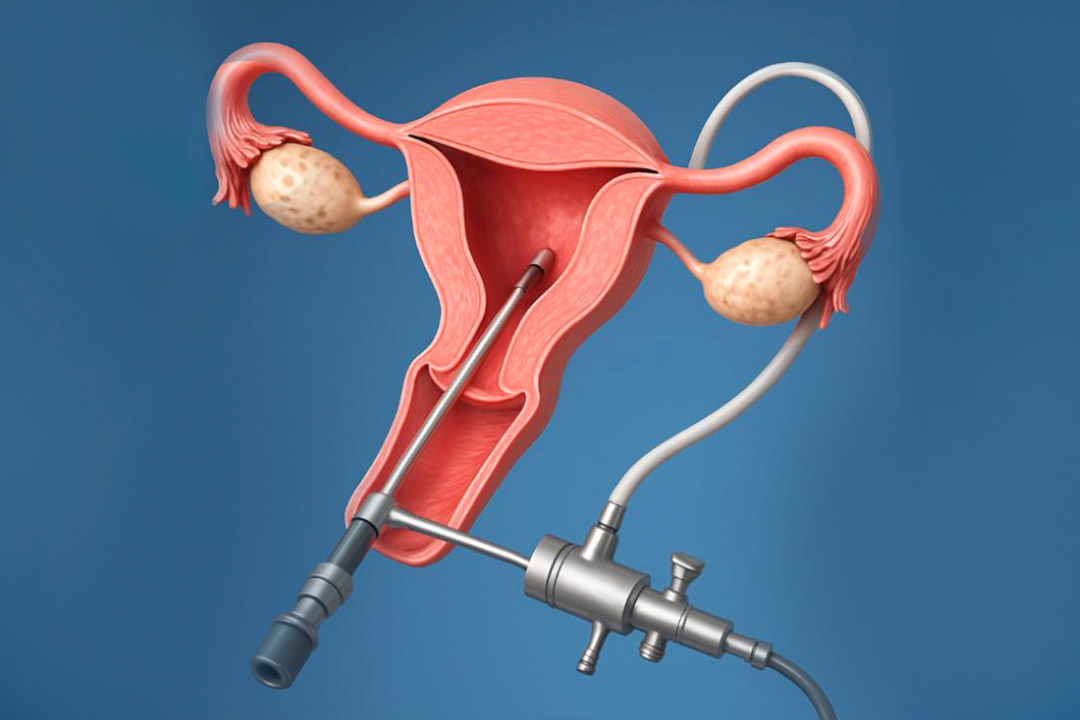
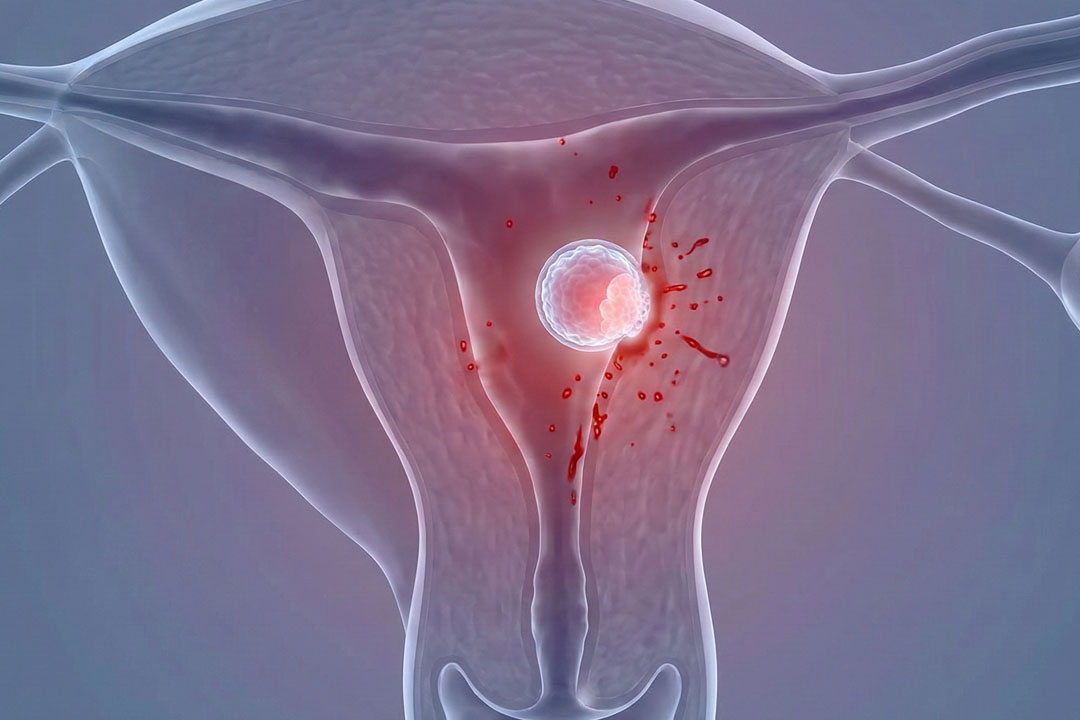
Hysteroscopy lets a clinician see the uterine cavity in real time using a narrow scope with a camera and light source.
Saline or a similar fluid is used to gently expand the cavity so the lining and the openings of the fallopian tubes can be seen clearly.
Instruments can be threaded through the scope to remove polyps, shave submucosal fibroids, release scar tissue (adhesions), or sample tissue.
Why is Hysteroscopy Done?
Common reasons include:
- Heavy or prolonged periods
- Bleeding between periods
- Bleeding after menopause
- Suspected polyps or fibroids
- Possible uterine adhesions (Asherman’s syndrome)
- Uterine septum
- Retained tissue after birth or miscarriage
- To locate or remove an intrauterine device
It may also be suggested as part of fertility work-ups or after repeated miscarriages.
Diagnostic vs Operative Hysteroscopy
A diagnostic hysteroscopy focuses on inspection and minor sampling to confirm what’s causing symptoms. An operative hysteroscopy goes a step further: once a problem is seen, small instruments are used through the same scope to treat it.
It helps with removing polyps, shaving fibroids, cutting adhesions, or, in some cases, performing procedures like endometrial ablation (when appropriate for heavy bleeding). Many services combine both in one visit to avoid a second procedure.
When is Hysteroscopy Usually Scheduled?
If cycles are regular, it’s often booked for the first week after a period ends to give the clearest view. This timing keeps the lining thin and reduces the chance that blood or mucus will obscure the view. If cycles are irregular or if you’re post-menopausal, the timing is arranged individually.
Preparation for Hysteroscopy
Preparation is simple: share your medication list, follow fasting instructions if anesthesia is planned, and arrange a ride home if you’ll be sedated.
You may be asked to pause blood-thinning medicines in advance. A brief exam or pregnancy test may be done the day of the procedure. Follow any specific advice you’re given about food, fluids, and comfort measures.
Hysteroscopy Procedure Step-by-Step
Below is a typical flow for an outpatient or day-surgery hysteroscopy. Details vary depending on whether it’s purely diagnostic or also operative.
Arrival and checks
You sign in, review consent, and confirm your plan. If sedation or general anesthesia is planned, an anesthesia professional will meet you first. You’ll change into a gown and empty your bladder.
Positioning
You lie on the exam table with legs supported, similar to a routine pelvic exam. A brief pelvic exam may be performed.
Anesthesia or comfort measures
Depending on the setting and scope of work, you may have a local numbing medicine on the cervix, oral or IV sedation, regional anesthesia, or general anesthesia. The goal is to keep you comfortable and still.
Gentle cervical access
A speculum may be used. The cervix is cleaned. If needed, it’s dilated slightly to allow the scope to pass. Many diagnostic procedures use very thin scopes and minimal or no dilation.
Scope insertion
The hysteroscope is a slim, lighted tube which is guided through the cervix into the uterine cavity. A clear fluid is circulated to open the space and wash away bubbles or mucus so the entire lining can be seen.
Full inspection
The clinician inspects the lining, the uterine shape, and the tubal openings. The camera sends images to a screen, helping identify polyps, submucosal fibroids, adhesions, septa, or retained tissue. If only a look is needed, this part can be very brief.
Treatment if needed (operative stage)
Through the scope, slender tools can remove a polyp (polypectomy), shave a small fibroid (myomectomy), cut scar bands (adhesiolysis), or perform other targeted treatments. This “see and treat” approach can save a second appointment.
Completion
The fluid is stopped, instruments are removed, and you’re moved to recovery. Diagnostic hysteroscopy may take only a few minutes but operative procedures can take longer, especially if multiple findings are treated at once.
How Long Does a Hysteroscopy Take?
It can be as quick as 5–10 minutes for a simple diagnostic look, or up to an hour or so if treatment is done at the same time. If another planned procedure is added such as laparoscopy then the total time is longer.
What are the Risks of Hysteroscopy?
Hysteroscopy is considered very safe and significant complications are uncommon. Possible issues include:
- Infection
- Heavier-than-expected bleeding
- Fluid-related problems
- Faintness
- Injury to the uterus or nearby organs
Diagnostic procedures have very low complication rates. Operative procedures carry a slightly higher risk, which rises with complexity (for example, large fibroid removal or extensive adhesiolysis). Your team counters these risks with careful technique and fluid monitoring.
Call your doctor if you develop a fever, severe abdominal pain, very heavy bleeding, or symptoms that worry you. These signals deserve prompt attention to rule out infection or a rare complication.
Is Hysteroscopy the Same as a D&C or Ablation?
No, these are different tools and goals, though they may be done in the same session.
A D&C gently scrapes the lining to collect tissue when a larger sample is needed; ablation intentionally destroys the lining to reduce heavy bleeding.
Hysteroscopy adds direct vision and precise, targeted treatment through the scope.
Frequently Asked Questions
Will hysteroscopy help with heavy periods?
Yes, if a structural cause is found, it can often be treated on the spot. Polyps can be removed and certain fibroids can be shaved down during the same procedure. If bleeding is due to hormonal or other non-structural reasons, your clinician may recommend medical therapy instead.
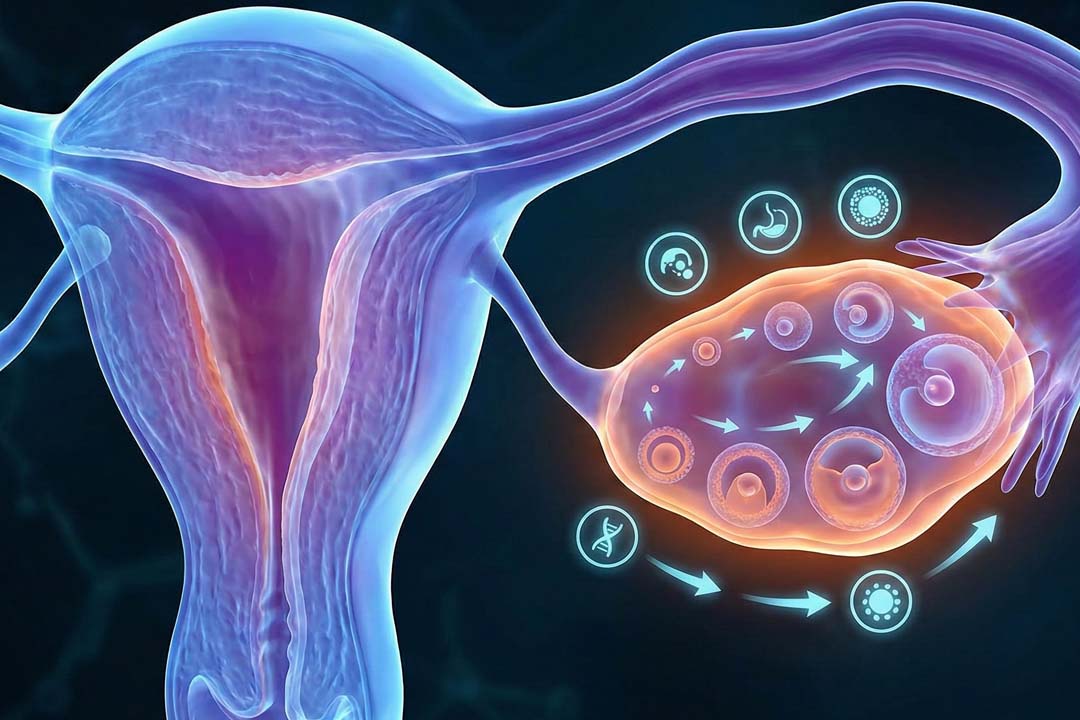
Can hysteroscopy improve fertility?
It can, when the barrier to pregnancy is inside the uterus and removable. Taking out a polyp, dividing adhesions, or correcting a septum may improve the chance of implantation. Your overall fertility plan will still consider age, egg quality, sperm factors, and other findings.
How soon can I try to conceive after hysteroscopy?
Your clinician will guide you, but many people wait until bleeding has stopped and the lining has healed, which may be one cycle. If extensive treatment was performed, more healing time may be advised. Always check your specific plan. (General recovery guidance after hysteroscopy supports a brief rest period while spotting settles.)
Can I drive myself home after hysteroscopy?
Only if you did not receive sedation and feel well; otherwise, arrange a ride. Sedation or general anesthesia affects reaction time, so you’ll be told not to drive for a period after the procedure.
How will my period change after hysteroscopy?
Light spotting for up to a week is common; your next period may be slightly earlier, later, lighter, or heavier depending on what was done. After minor diagnostic procedures, cycles usually return to baseline quickly. After polyp removal or other treatment, flow may improve over time.
How does hysteroscopy differ from hysterosalpingography (HSG)?
HSG is an X-ray dye test that checks if fallopian tubes are open while hysteroscopy is a direct look inside the uterus and can also treat problems. They answer different questions and are sometimes used together in a fertility assessment.
Can endometrial ablation be done during hysteroscopy?
Yes, ablation is often guided by hysteroscopy, but it’s only for people who are done with childbearing. Its goal is to reduce or stop heavy bleeding by destroying the uterine lining. Your clinician will review benefits, limits, and alternatives.
Is Hysteroscopy painful?
Experiences vary, but most people describe cramping similar to period pain; stronger pain relief or anesthesia is used when more extensive work is planned. Prior births, procedure length, and anxiety can influence how it feels. Speak up about comfort; the team can tailor pain control to you.
Conclusion
Hysteroscopy offers clear answers and targeted treatment through a small, natural opening rather than an incision.
For many people, it explains why bleeding is irregular or heavy and fixes the cause in one visit. Preparation is straightforward, the steps are predictable, recovery is usually quick, and complications are uncommon.
If hysteroscopy has been recommended for you, ask about timing, anesthesia options, and whether treatment is likely at the same time as diagnosis. A short, well-planned procedure today can spare you repeated tests and help you feel better sooner.
About Us
AKsigen IVF is a premier center for advanced fertility treatments, with renowned fertility experts on our team. Specializing in IVF, ICSI, egg freezing, and other cutting-edge reproductive technologies, AKsigen IVF is committed to helping couples achieve their dream of parenthood. With personalized care and a patient-first approach, AKsigen IVF provides comprehensive fertility solutions under one roof.