What are the Hormone Tests for Female Fertility?: Types, Purpose & Normal Levels
Trying to conceive can feel like a complicated task. When pregnancy doesn’t happen as quickly as expected, hormone testing is often one of the first tools clinicians use to understand what’s going on.
These blood tests look at the chemical “messengers” that drive egg maturation, ovulation, uterine preparation, and other steps required for conception..
This guide explains the core hormone tests used in female fertility care, what each one shows, and how results are interpreted alongside your history.
You’ll also find practical notes on timing, how birth control can affect results, and India-specific FAQs (including approximate costs in INR).
How Clinicians Choose Your Hormone Tests?
The goal is to answer three questions:
(1) Are you ovulating?
(2) What is your ovarian response likely to be if you need treatment?
(3) Are there correctable hormonal conditions like thyroid or prolactin issues affecting cycles?
Professional guidance emphasizes changing tests to history and cycle patterns, not ordering everything for everyone. For example, mid-luteal progesterone confirms ovulation; early-cycle FSH/estradiol or AMH gauge ovarian reserve; and TSH/prolactin are checked when symptoms or cycle irregularity suggest a problem.
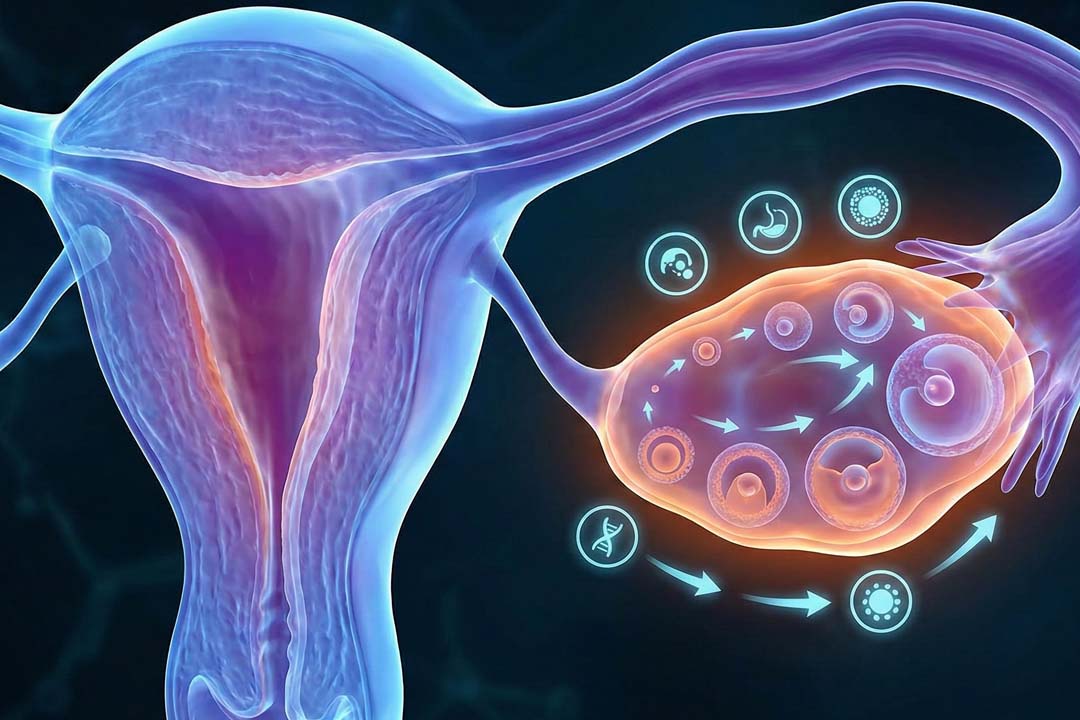
Ovulation: Mid-luteal progesterone rises
A mid-luteal progesterone blood test (commonly nicknamed the “day-21 test,” but better timed as ~7 days after ovulation) confirms that ovulation occurred. Progesterone peaks six to eight days post-ovulation; the exact calendar day varies with cycle length, so timing the test to your luteal phase rather than a fixed day is more accurate.
If your cycles are irregular, your clinician may pair bloodwork with ovulation-tracking methods or ultrasound to time the draw correctly.
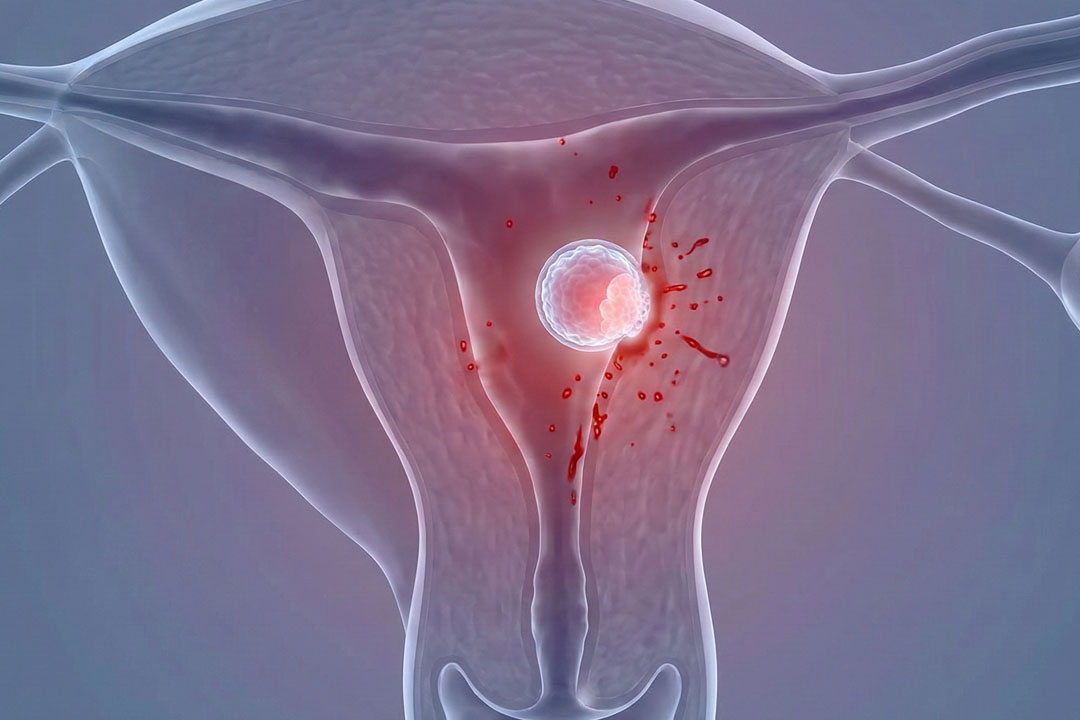
Adequate progesterone means an egg was released and the uterine lining received the hormonal signal to prepare for implantation. Persistently low values suggest anovulation (no egg release) in that cycle and prompt further evaluation or ovulation induction strategies.
Ovarian Reserve Testing
Ovarian reserve tests estimate how the ovaries may respond to stimulation; they do not directly predict your ability to conceive naturally. The two most used are anti-Müllerian hormone (AMH, any day of the cycle) and a day-2–4 pair of FSH and estradiol.
AMH and antral follicle count (seen on ultrasound) are strong indicators of expected egg yield in IVF, while day-3 FSH/E2 provide a traditional check on early-cycle signaling. However, low AMH alone does not mean you cannot get pregnant without treatment; its predictive value for natural conception is limited.
Reserve testing helps set realistic expectations, individualize medication doses, and flag extremes (very low response or risk of over-response). Current guidance stresses using AMH/AFC primarily to counsel about stimulation and retrieval numbers, not to forecast whether you will conceive on your own or to screen people not seeking fertility care.
Few Factors to Consider
Timing: AMH can be drawn any cycle day; FSH/E2 are best days 2–4 to interpret baseline pituitary–ovarian tone. Elevated day-3 estradiol can “mask” FSH and still suggest diminished reserve.
Contraceptives: Combined hormonal contraception can lower AMH transiently; results should be interpreted with method use in mind. (Your clinician may repeat testing after a washout if needed.)
LH and Ovulation Predictor Kits
Urine LH kits detect the pre-ovulatory surge to time intercourse/IUI but are not diagnostic of broader fertility problems.
In irregular cycles or polycystic ovary syndrome (PCOS), elevated baseline LH can make kits less reliable; pairing with ultrasound or serum progesterone confirmation improves accuracy. Clinical guidance treats LH kits as adjuncts for timing rather than stand-alone tests.
Thyroid Function Tests
A TSH (and, when indicated, free T4) checks for hypo- or hyperthyroidism that can disturb ovulation, luteal function, and miscarriage risk.
Subclinical thyroid problems sometimes show up first as cycle changes or difficulty conceiving; treating overt thyroid disease benefits overall reproductive outcomes. TSH is a standard part of the work-up when history or symptoms point that way.
Prolactin Level
An elevated prolactin level can disrupt the normal GnRH-LH/FSH pulses and lead to irregular cycles or anovulation.
Testing is usually done in the morning, ideally fasting and avoiding breast stimulation/exam just before the draw; significantly high results are repeated and evaluated for physiologic, medication-related, thyroid, renal, or pituitary causes. Treating the underlying cause often restores ovulation.
Androgen Profile
If you have excess hair growth, acne, or very irregular cycles, clinicians may check total/free testosterone, DHEA-S, and sometimes 17-hydroxyprogesterone. The aim is to distinguish common PCOS from less common adrenal or ovarian androgen excess.
Addressing androgen-related cycle dysfunction can improve ovulation frequency and pregnancy chances, either spontaneously or with ovulation induction.
Estradiol Across the Cycle
Besides day-3 estradiol (interpreted with FSH), mid-cycle estradiol helps track follicle growth during treatment cycles.
As a diagnostic tool outside treatment, estradiol is most informative when paired with timing, ultrasound findings, and other hormones rather than used alone. Guidance does not recommend estradiol as a single predictor of natural fertility outcomes.
Putting the Panel Together
Different circumstances require different strategies, for instance:
- Regular cycles, <35 years, trying for more than 12 months: Mid-luteal progesterone to confirm ovulation; consider TSH and prolactin based on symptoms; reserve testing if treatment is being planned or to anticipate response.
- Irregular or absent periods: Check TSH, prolactin, FSH/LH (and androgens if PCOS suspected); confirm if/when ovulation occurs; reserve tests as indicated for planning.
- Planning IVF or egg freezing: AMH and/or AFC plus day-3 FSH/E2 guide dosing and expectations.
What if my Hormone Tests Show Abnormal Results?
Abnormal results guide targeted action to treat correctable conditions (thyroid disease, hyperprolactinemia), address lifestyle or medication factors, and choose appropriate fertility treatment (e.g., ovulation induction for anovulation.
IVF with tailored stimulation for low or high ovarian response). The interpretation is always personalized, and one off-range number rarely tells the whole story.
When an IUD or Hormonal Contraception is in Place
Hormonal IUDs and pills can alter bleeding patterns and some lab values (notably AMH) while you’re using them, which complicates interpretation. If you’re evaluating ovulation or reserve while on contraception, your clinician will decide whether to test now (with caveats) or pause the method and retest after a washout period. Copper IUDs have fewer hormonal effects but can still complicate timing of certain tests.
What Hormone Tests Cannot Do
Hormone tests are very useful but it is important to know to what extent, for instance:
- Guarantee natural conception: Low AMH does not automatically mean you can’t conceive on your own; high AMH does not guarantee quick conception.
- Replace age as a key factor: Age remains the most powerful predictor of egg quality and overall chances per cycle. Reserve tests are complements, not substitutes.
Frequently Asked Questions
When to consider IVF treatment?
If you’ve been trying for 12 months with regular cycles (or 6 months if you’re ≥35), see a fertility specialist for evaluation. Many 30-year-olds conceive with simpler treatments (cycle tracking, ovulation induction, IUI) once a specific issue is addressed; IVF is reserved for indications like blocked tubes, severe male factor, or when time is a priority.
Do I need to stop my IUD or pills to test hormones?
Not always, but hormonal methods can lower AMH and obscure ovulation timing. Your clinician may interpret with caution or ask for a short washout before retesting. Copper IUDs have fewer hormonal effects.
Can blood tests alone diagnose PCOS?
Diagnosis relies on a combination of irregular ovulation, clinical/biochemical signs of androgen excess, and polycystic morphology on ultrasound (after excluding other causes). Blood tests (androgens, sometimes 17-hydroxyprogesterone) support the diagnosis but are not the sole criterion.
If my AMH is low, should I rush into IVF?
Not automatically. Low AMH suggests fewer recruitable follicles for stimulation, which can influence treatment planning, but it doesn’t rule out natural conception. Discuss age, timeline, tube status, semen parameters, and your goals before choosing a pathway.
Is “luteal phase defect” a common cause of infertility that needs routine treatment?
Short luteal phases and low mid-luteal progesterone occur in some cycles, but definitions and testing thresholds are debated. Management focuses on improving ovulation quality and addressing underlying issues; progesterone support is targeted, particularly in assisted reproduction or recurrent miscarriage contexts.
How long should we try before testing?
12 months if you’re <35, 6 months if ≥35, or earlier if you have irregular cycles, known pelvic disease, or a history suggesting reduced fertility. Male-factor testing should proceed in parallel.
Conclusion
Hormone testing doesn’t give a single yes-or-no answer but it pieces together the story of how your cycle is working. Mid-luteal progesterone confirms ovulation, AMH and day-3 FSH/E2 guide expectations for treatment response, and thyroid or prolactin checks uncover correctable issues that may be getting in the way.
Interpreted alongside age, ultrasound findings, and a semen analysis, these results help your clinician recommend the simplest, most effective next step whether that’s cycle tracking, ovulation induction, IUI, or IVF. If something looks off, it’s a starting point for action, not a dead end.
About Us
AKsigen IVF is a premier center for advanced fertility treatments, with renowned fertility experts on our team. Specializing in IVF, ICSI, egg freezing, and other cutting-edge reproductive technologies, AKsigen IVF is committed to helping couples achieve their dream of parenthood. With personalized care and a patient-first approach, AKsigen IVF provides comprehensive fertility solutions under one roof.