What is Blastocyst Culture?
Many people start learning about IVF by hearing terms like “day-3 embryos,” “day-5 transfer,” or “blastocyst.” It can feel like a new language when you’re already juggling appointments, injections, and hope.
Blastocyst culture is simply a way of growing embryos in the lab for a little longer, usually to day 5 or day 6 after fertilisation, so the embryology team can see which ones continue to develop well. This extra time helps with selection and often allows doctors to transfer just one strong embryo while keeping the chance of pregnancy high and the risk of twins low.
Not every patient needs it, and not every IVF cycle is suited to it, but for many, it’s become a standard part of modern IVF because it improves decision-making at transfer.
What Exactly is Blastocyst Culture?
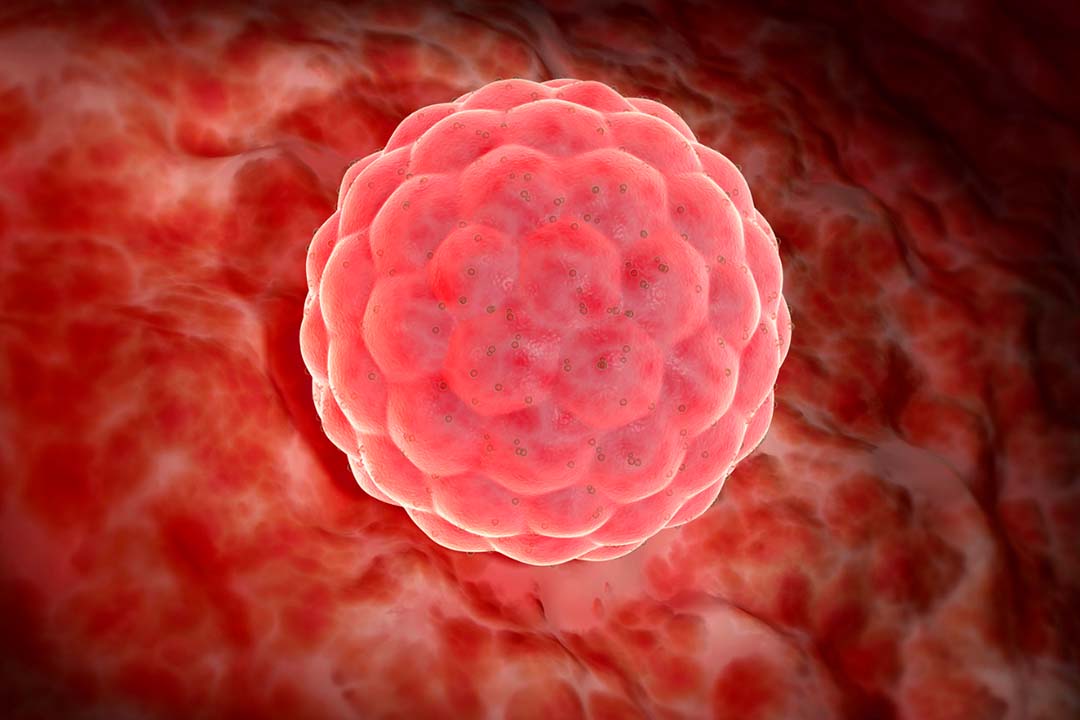
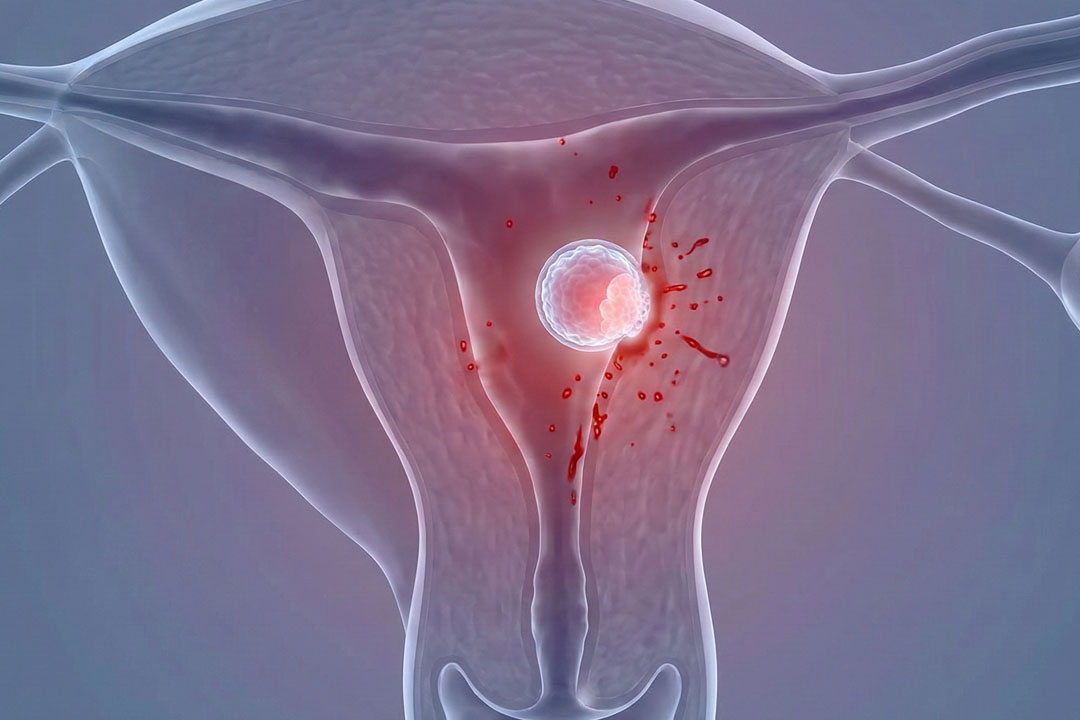
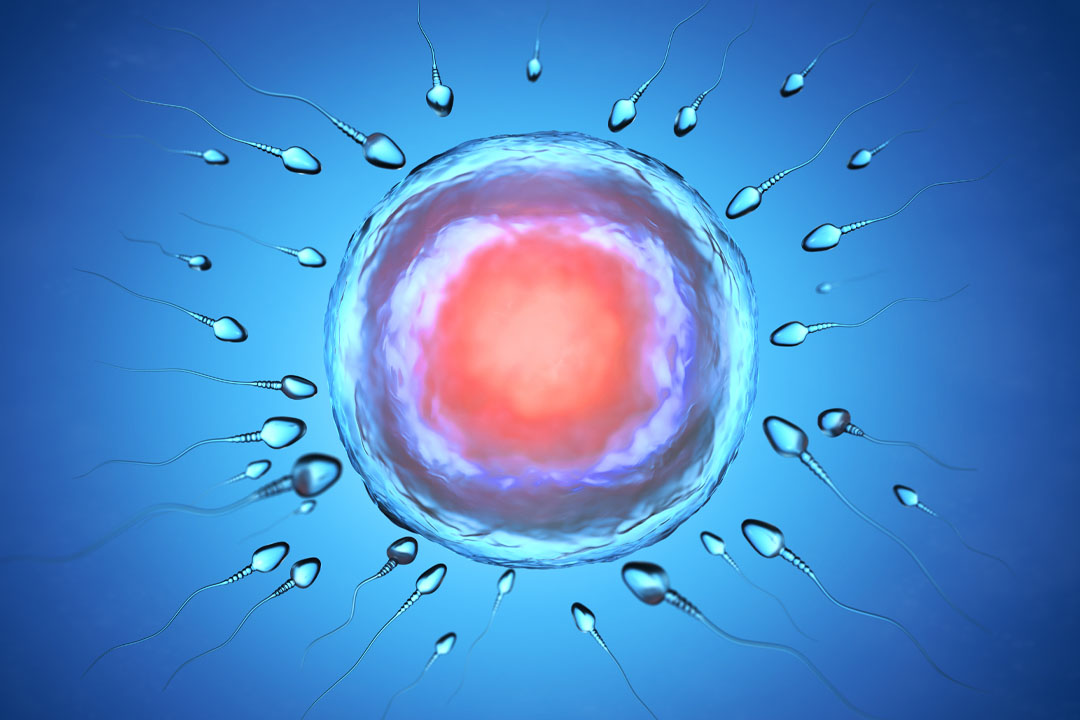
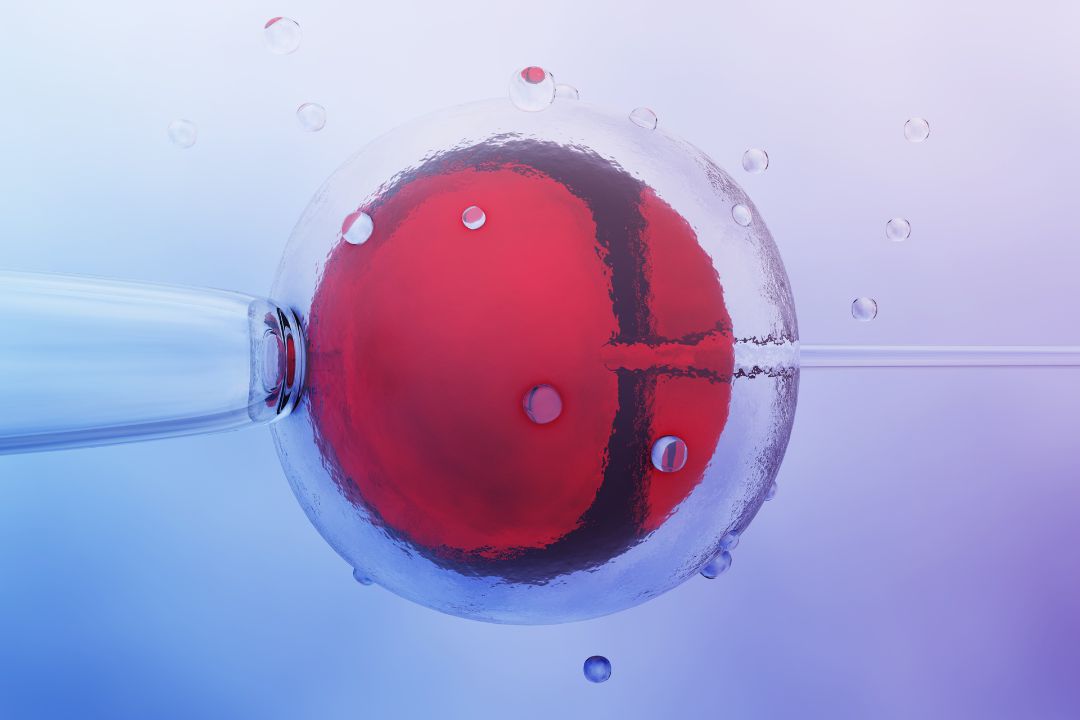
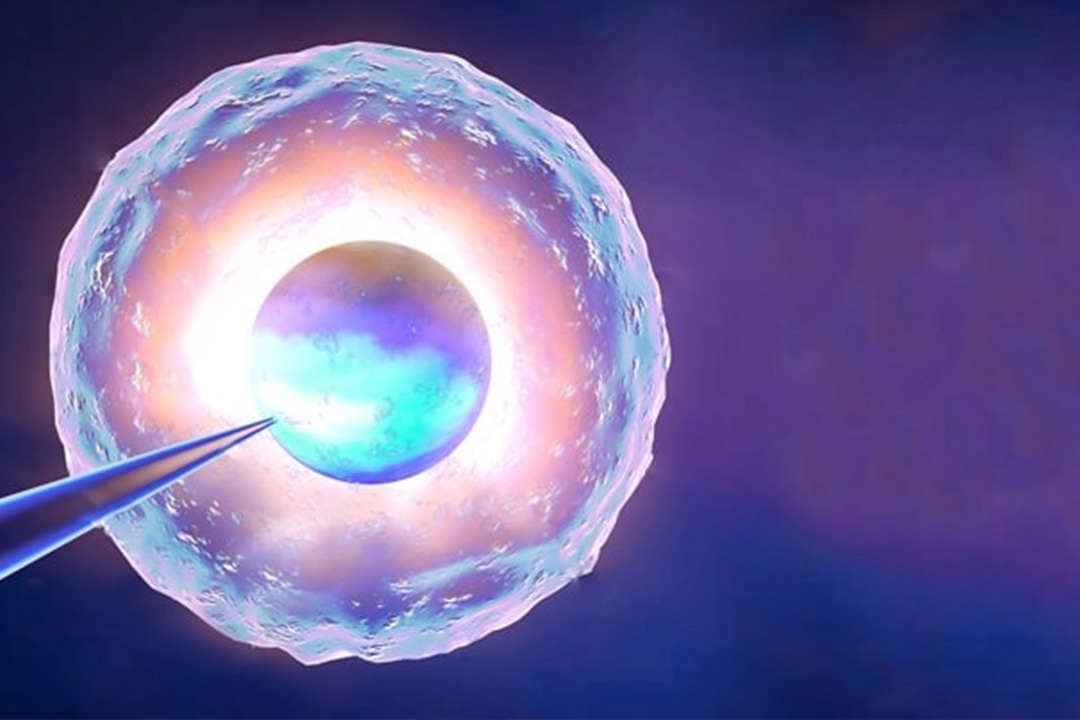
Blastocyst culture means keeping embryos in the lab until they reach the “blastocyst” stage, usually on day 5 or 6, instead of transferring them earlier on day 2 or 3. At this point the embryo has hundreds of cells and two clear parts: the inner cell mass (which becomes the fetus) and the trophectoderm (which becomes the placenta).
Growing embryos to this stage uses specialised culture media, stable temperature and pH control, and careful observation. The goal is simple: identify embryos that show ongoing growth and organisation, because those are more likely to implant after transfer. PMC
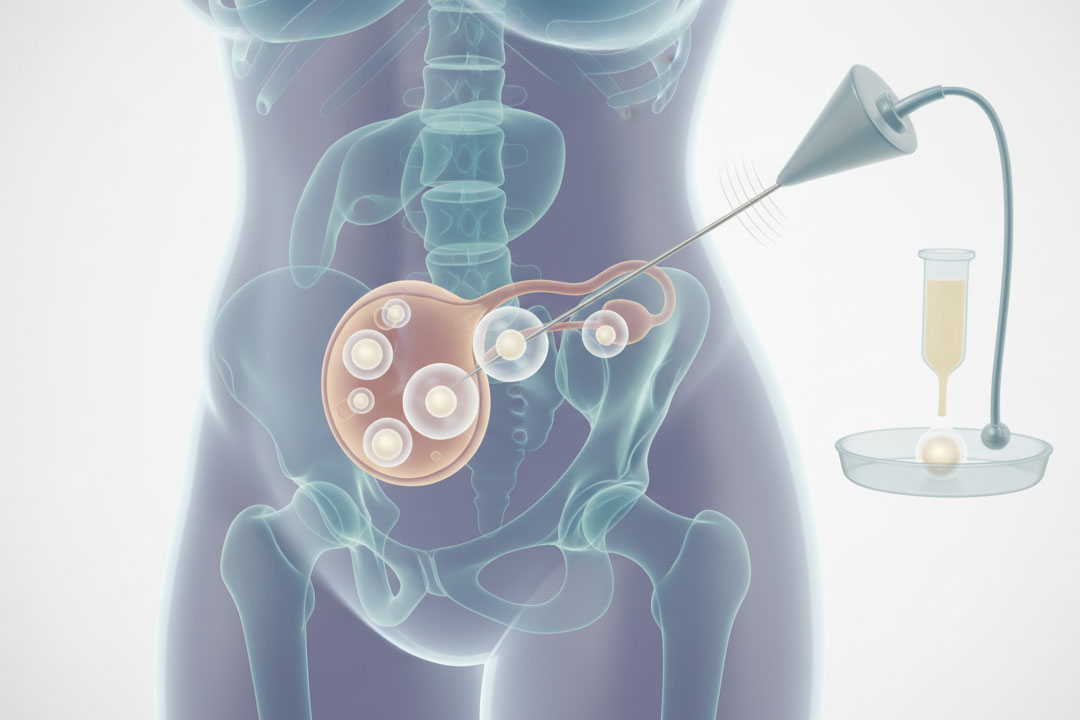
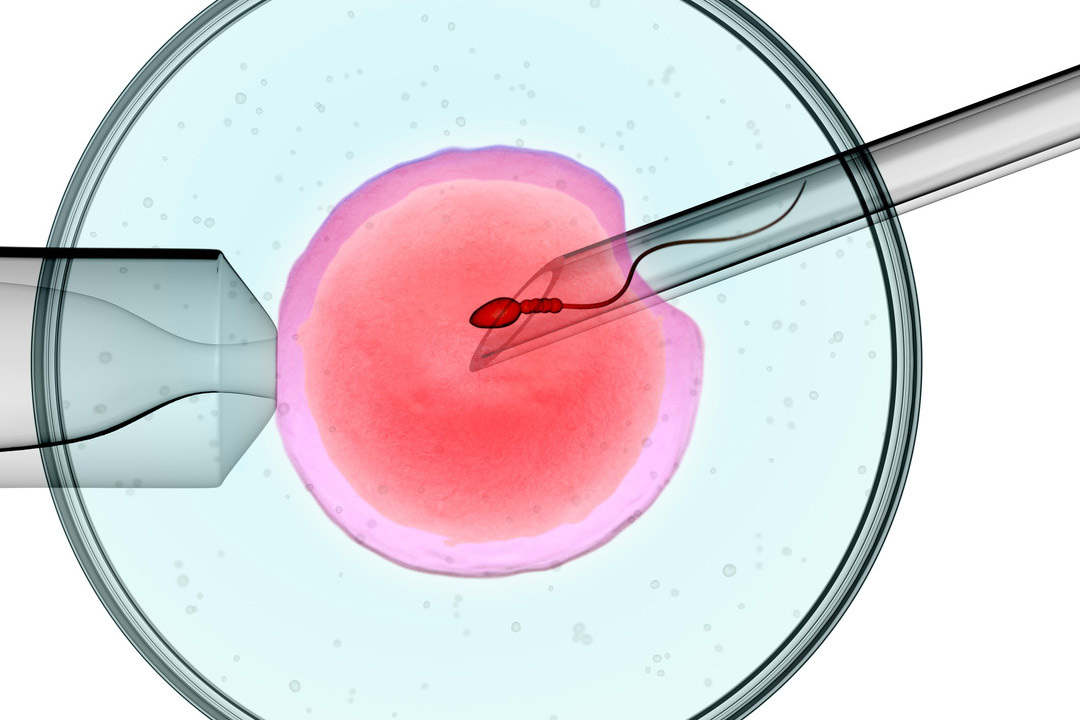
How Does the Lab Grow Embryos to Day 5 or 6?
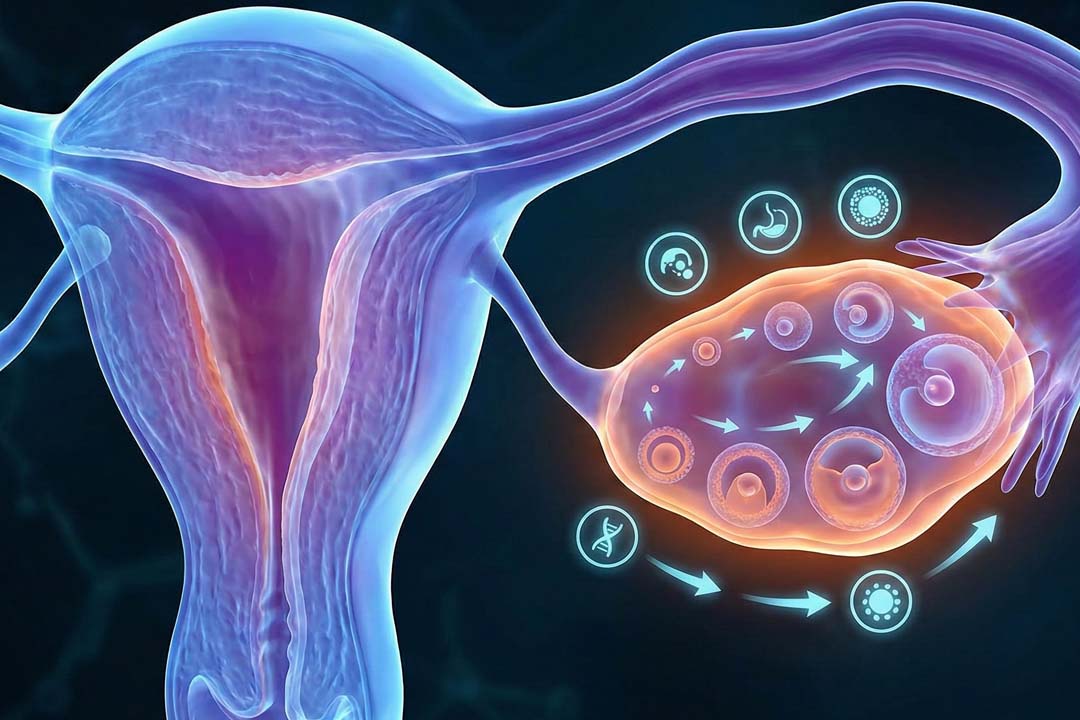
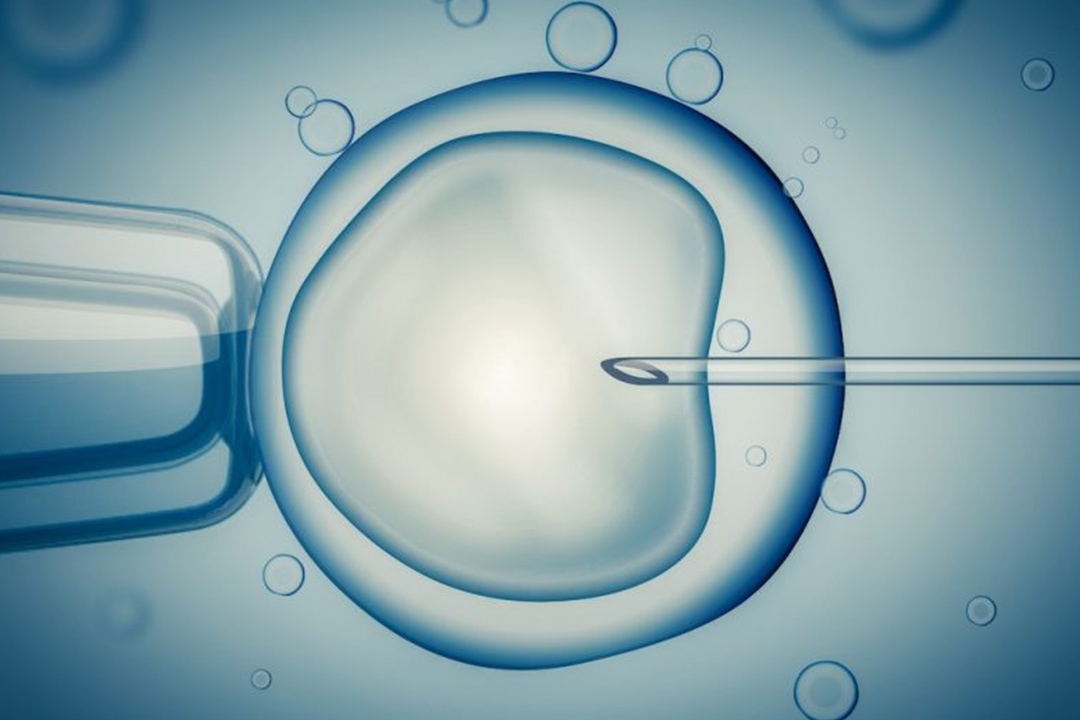
Embryos are placed in drops of culture media and kept in small, controlled incubators that hold temperature and gases steady.
Embryologists check development at planned intervals, looking for cell division patterns on day 2 and day 3 and then for a fluid-filled cavity and a well-formed inner cell mass by day 5 or 6.
Some clinics use time-lapse systems so embryos can be observed without removing them from the incubator. When a blastocyst looks ready, it can be transferred fresh or frozen for a future cycle.
Why do Clinics Use Blastocyst Culture?
The main reason is better selection by day 5/6, the embryos that keep growing have shown more developmental potential, so one well-chosen blastocyst can carry a strong chance of success.
This lets many patients have a single-embryo transfer without lowering their odds, which helps avoid twins and triplets. Several large reviews and agencies note higher pregnancy rates per fresh transfer with blastocyst-stage embryos compared with day-2/3 embryos.
Day-3 vs. Day-5: What’s the Real Difference?
On day 2 or 3 (the “cleavage” stage), embryos have only a handful of cells, so it is harder to tell which ones will keep going. On day 5 or 6, a blastocyst has expanded, started to form a cavity, and shows clearer structure. That visible progress helps with selection and often translates into better implantation per transfer.
However, there is a trade-off: by waiting until day 5/6, some embryos stop growing in the lab, which can reduce how many you have available overall. This is why your team will balance embryo numbers, your age, egg quality, and your history when choosing between day-3 and day-5 plans.
Does Blastocyst Culture Improve Success Rates?
Per fresh transfer, many studies show a higher chance of ongoing pregnancy or live birth with a single blastocyst compared with a single cleavage-stage embryo. A recent review summarised that fresh blastocyst transfers may lead to more live births than fresh cleavage-stage transfers.
That said, because fewer embryos may reach day 5/6, the cumulative chance of a baby from one egg collection (counting fresh and all frozen transfers) can be similar between the two strategies for some patients. This is why the decision is personalised rather than automatic.
Does Blastocyst Culture Lower the Risk of Multiple Pregnancy?
Yes, by supporting single-embryo transfer (SET) without reducing success for many patients.
Professional guidelines encourage SET in suitable cases, and they specifically state that when a chromosomally normal (euploid) embryo is available, only one should be transferred regardless of age.
Reducing the number of embryos transferred is the most effective way to avoid twins, which carry higher health risks for both the pregnant person and the babies.
What are the Advantages of Blastocyst Culture?
There are several advantages of Blastocyst Culture:
- Sharper embryo selection
Letting embryos reach day 5/6 helps spot the ones that keep developing well, which usually boosts implantation per transfer. - Better timing with the uterus
A day-5 transfer lines up more closely with when an embryo naturally reaches the uterus, improving endometrium–embryo sync. - Supports single-embryo transfer
Because selection is stronger, clinics can transfer one good blastocyst and still keep success high by cutting twin/triplet risk. - PGT-friendly
The blastocyst stage is ideal for biopsy (a few trophectoderm cells), so genetic testing slots neatly into the workflow.
What are the Risks of Blastocyst Culture?
The main downside is that some cycles may end with few or no blastocysts to transfer, especially when egg numbers are low. Waiting until day 5/6 means some embryos are arrested before transfer, and in a small share of cycles, there may be nothing suitable to move or freeze.
A few studies have also suggested slightly different perinatal patterns after blastocyst transfer (for example, preterm birth) compared with cleavage-stage transfer, though findings are mixed and still being studied. Your doctor will weigh these factors against the potential gains in selection.
Who is a Good Candidate for Blastocyst Culture?
People with a reasonable number of good-quality embryos on day 3 often benefit most from extending culture to day 5/6. In such cases, the chance of having blastocysts to choose from is higher, which makes selection and SET practical. This approach is very common worldwide and is supported by both professional societies and national regulators.
Who Might be Advised to Transfer Earlier?
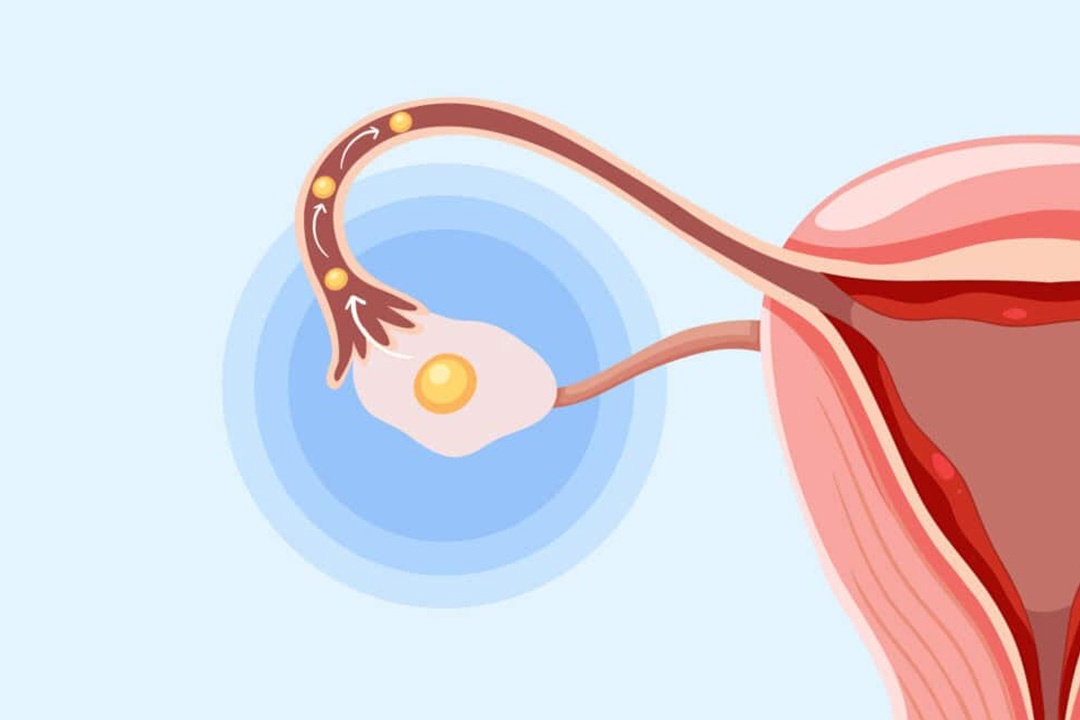
If only a few embryos are developing on day 2/3, an earlier transfer may be suggested to avoid the risk that none reach the blastocyst stage in the lab.
In these situations, the uterus provides the natural environment while the embryos continue to grow inside the body.
Your team will explain the pros and cons in your specific case, including your age, egg quality, and any previous cycle outcomes.
Fresh Versus Frozen Blastocyst Transfer
Many clinics now freeze (vitrify) blastocysts and transfer in a later cycle because it can simplify timing and allow the endometrium to be prepared calmly. Others still perform fresh transfers when hormone levels and lining look good.
Survival after vitrification is high in modern programs, and some centres will thaw day-3 embryos and grow them to day 5 before transfer in frozen cycles when that improves selection. Your clinic will choose the sequence that best fits your medical picture and lab practice.
Does Blastocyst Culture “select” for Genetically Healthier Embryos?
Not directly, but it helps identify embryos with better developmental potential, which often correlates with chromosomal normality. True chromosome screening requires preimplantation genetic testing (PGT).
If PGT is part of your plan, biopsy is usually done at the blastocyst stage from the trophectoderm, and professional groups publish guidance on how to interpret those results (including “mosaic” findings).
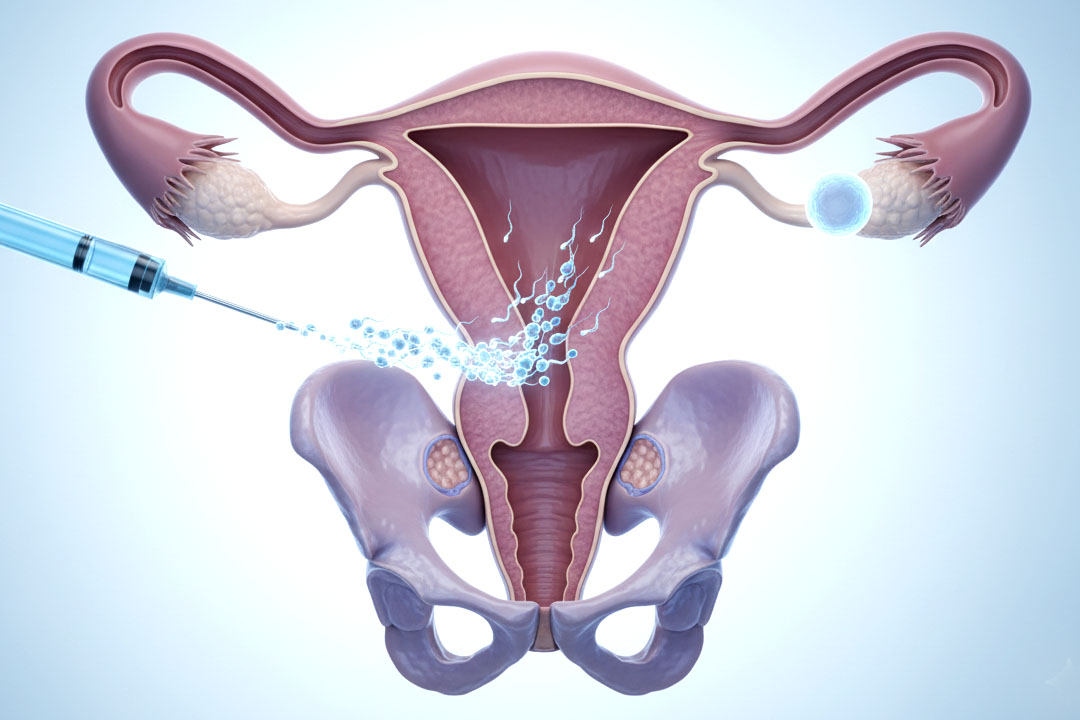
How many embryos should be transferred with blastocyst culture?
Professional guidance is clear: transfer one embryo in most cases; transfer of more than one is generally reserved for specific situations after careful counselling. If genetic testing shows a euploid blastocyst, guidance recommends transferring one regardless of age. The aim is to maintain success while avoiding the extra risks tied to multiple pregnancy.
Frequently Asked Questions
Is blastocyst transfer more successful than day-3 transfer?
Per fresh transfer, many studies show higher pregnancy and live-birth rates with blastocysts than with cleavage-stage embryos. Keep in mind the whole picture: some people may have fewer embryos left to freeze, which can even out total success across all transfers from the same egg collection.
Will blastocyst culture increase my chance of twins?
No, quite the opposite, because it supports single-embryo transfer without sacrificing success for many patients. Transferring one embryo is the key step to avoid multiples.
What if none of my embryos reach day 5 or 6?
That can happen, especially when starting with a small number of eggs or embryos. Your team may suggest transferring earlier in future cycles or adjusting stimulation, lab conditions, or strategy based on what they learn from your cycle.
Is a day-6 blastocyst worse than a day-5 blastocyst?
Not necessarily. Day-6 blastocysts can and do lead to healthy pregnancies. Embryologists look at expansion, inner cell mass, and trophectoderm quality, not just the day number when choosing which embryo to transfer or freeze.
Does blastocyst transfer change the risk of birth defects?
Current data do not show a clear increase in congenital anomalies from transferring blastocysts compared with cleavage-stage embryos. Some studies explore differences in preterm birth or birthweight across strategies; your doctor will discuss context for your case.
Is blastocyst culture required if I plan to do PGT?
Usually, yes. Biopsy for PGT-A/M is most often performed at the blastocyst stage by removing a small number of trophectoderm cells, and most centres use this approach.
Will I still need bed rest after a blastocyst transfer?
No special bed rest is required. Normal gentle activity is fine unless your doctor advises otherwise for a separate reason.
Does blastocyst culture change how many embryos I’ll have to freeze?
Possibly. Because some embryos stop growing before day 5/6, you might end up with fewer frozen embryos than if you had transferred or frozen earlier. On the flip side, those that do reach the blastocyst stage are more likely to be robust.
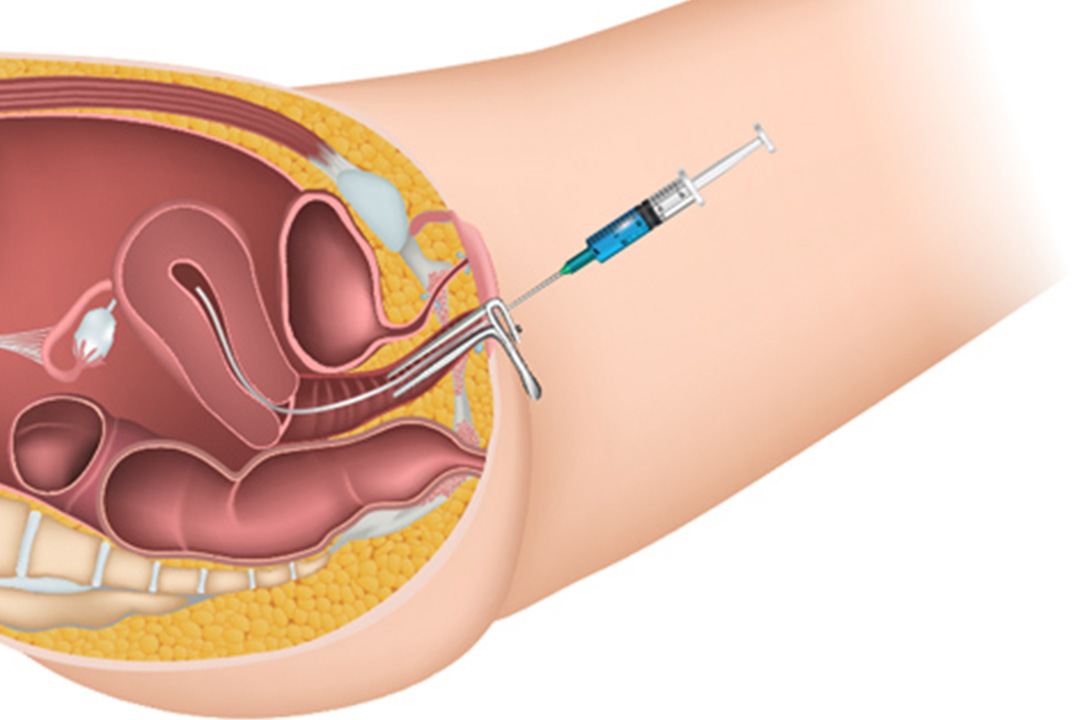
Does blastocyst transfer hurt?
The transfer itself is usually quick and feels similar to a Pap test for many people. It’s done without anaesthesia in most cases. Mild cramping can occur, but severe pain is uncommon; tell your team if you feel unwell.
Can I choose between fresh and frozen blastocyst transfer?
Often, yes. Your team will guide you based on hormone levels, lining quality, and your medical history. Both approaches are widely used, and frozen blastocyst transfers are very common today.
If I only make two embryos, should I still try for day-5?
Maybe not. With low embryo numbers, some clinics suggest an earlier transfer so the embryos can continue to develop in the uterus rather than risk arrest in the lab. This is a case-by-case call.
Conclusion
Blastocyst culture is a practical, widely used way to give embryos a little more time in the lab so the strongest ones can be seen and chosen. For many patients, this translates into higher success per transfer and a safer single-embryo approach that lowers the chance of twins.
The flip side is that waiting until day 5/6 can reduce how many embryos you ultimately have to transfer or freeze, and in some cycles there may be no blastocyst to move at all. The best plan is the one tailored to you as per your age, egg and embryo numbers, response to stimulation, and your history
About Us
AKsigen IVF is a premier center for advanced fertility treatments, with renowned fertility experts on our team. Specializing in IVF, ICSI, egg freezing, and other cutting-edge reproductive technologies, AKsigen IVF is committed to helping couples achieve their dream of parenthood. With personalized care and a patient-first approach, AKsigen IVF provides comprehensive fertility solutions under one roof.