Reproductive Age in Women: Key Stages, Fertility & Health Insights
The path to parenthood is rarely identical for any two people. Biology plays a role, but so do health, timing, life goals, finances, and family support. Broadly, a woman’s reproductive span begins after the first menstrual period (menarche) and ends with menopause. Yet within that long window, fertility isn’t a straightforward path.
It peaks, then gradually declines, and health risks shift with age. This article explains how age intersects with fertility and pregnancy outcomes, what “typical” reproductive ages look like, when to seek medical input, and the practical steps you can take to improve your chances of a healthy pregnancy whenever you’re ready.
Reproductive years, Menarche and Menopause
Most females start menstruating around early adolescence and reach menopause in midlife. Menarche commonly occurs close to age 12 (median ~12–12.5 years in large cohorts).
Menopause most often occurs between ages 45 and 55 (average close to 51–52 years). Together, these mark the broad bookends of the reproductive years, though the ease of conceiving changes across this span.
Fertility generally peaks in the late teens through the 20s, begins a slow decline around age 30, and the decline becomes steeper from the mid-30s onward.
By the early 40s, the monthly chance of pregnancy is much lower than in the 20s. These trends reflect a natural fall in both the number and quality of available eggs with age.
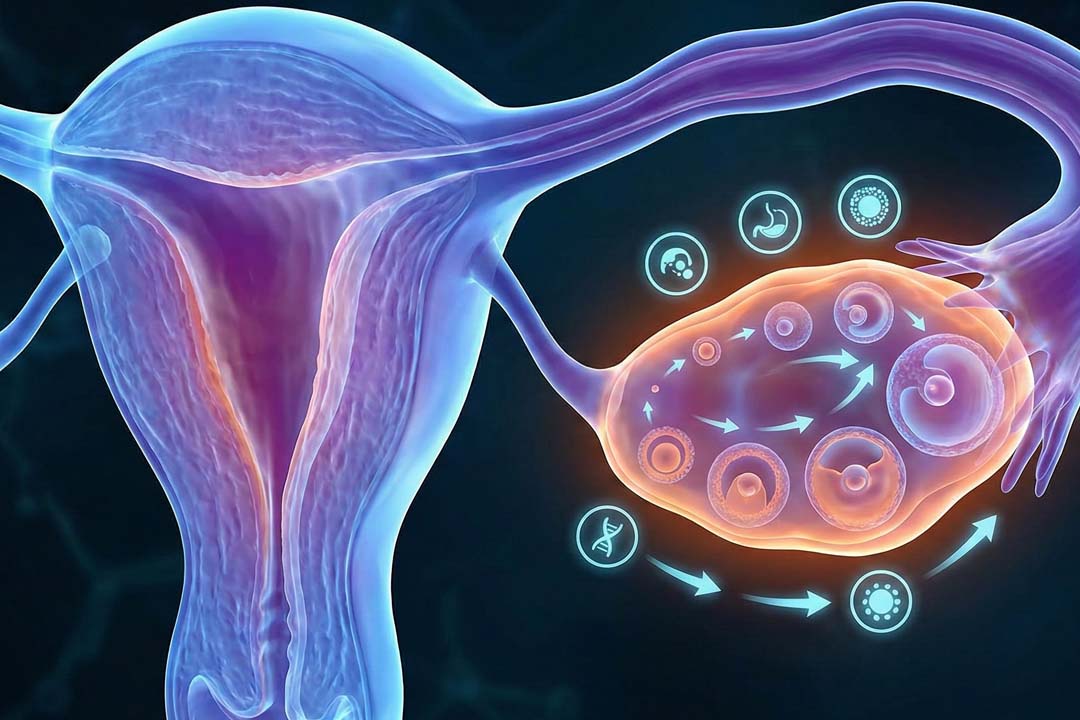
How Does Age Affect Egg Supply and Quality?
Women are born with a finite egg supply that steadily diminishes throughout life; egg quality also declines with time, which raises the risks of aneuploidy (chromosomal changes) and miscarriage. Medical societies emphasize this age-related decline, even as many pregnancies after 35 proceed safely with good care.
Age, Fertility, and Outcomes
Late teens and 20s are generally characterized by peak fertility, generally lower complication risks In this life stage, monthly chances of conception are the highest and pregnancy complications are typically fewer compared with later ages, assuming good overall health.
That doesn’t mean pregnancy is risk-free; it means the baseline probabilities are more favorable than they will be later.
Early 30s are mostly favorable, but the decline somewhat starts around this time. Fertility begins to taper in the early 30s. Many people still conceive naturally, but the monthly odds are lower than in the 20s, and some pregnancy risks (e.g., gestational diabetes, hypertensive disorders) start to inch upward with age.
Mid- to late-30s include steeper fertility decline and higher pregnancy risks. From about 35 onward, egg quality declines more quickly; miscarriage and chromosomal-condition risks rise with age, and complications such as gestational diabetes and preeclampsia are more common than in younger groups.
In 40s, possible, but typically harder to conceive.Natural conception is still possible in the early 40s, though the monthly chance is low compared with younger ages, and miscarriage risk is higher. Fertility treatments can help some people, but success rates also decline with advancing age.
What’s the Best Age to Get Pregnant?
Many experts consider the late 20s to early 30s a favorable window for overall outcomes, but the “best” age is personal and it depends on health, readiness, and life context. Some research modeling suggests optimal first-birth outcomes near age 30–31, yet this is a population statistic, not a rule for individuals.
What Age-Related Pregnancy Risks Should I Know?
Age-related pregnancy risks, particularly for women over 35, include an increased chance of miscarriage, gestational diabetes, high blood pressure like preeclampsia, and fetal chromosomal abnormalities such as Down syndrome. Other risks are preterm birth, low birth weight, and a higher likelihood of needing a cesarean delivery. For men over 40, there is an increased risk of certain genetic conditions in the offspring.
For the pregnant person
- High blood pressure and preeclampsia: The risk of high blood pressure and preeclampsia (a serious high blood pressure condition) increases with age. Preeclampsia can affect the growth of the baby and pose risks to the mother's health.
- Gestational diabetes: Older mothers have a higher risk of developing gestational diabetes, which can impact both the mother and baby.
- Multiple pregnancy: The likelihood of a multiple pregnancy increases with age because the ovaries may release more than one egg per month, and fertility treatments can also increase this risk.
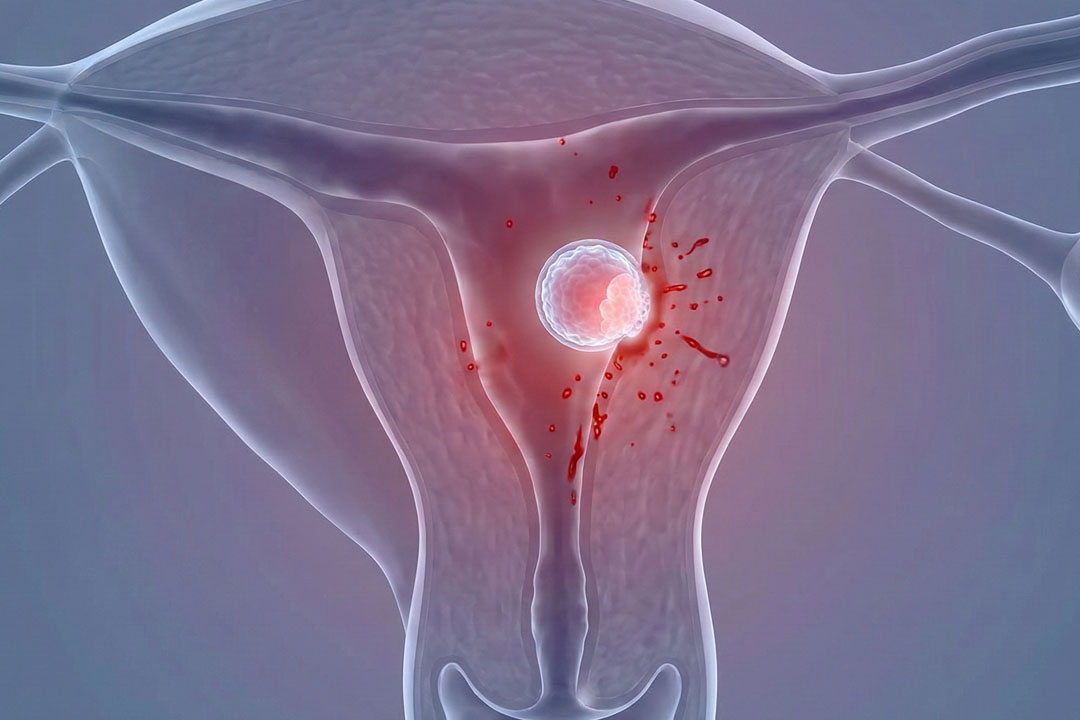
For the fetus
- Chromosomal abnormalities: The risk of the baby having a chromosomal abnormality, such as Down syndrome, increases with the mother's age.
- Pregnancy loss: The risk of miscarriage and stillbirth increases with age.
When to Seek a Fertility Evaluation
It is crucial to know when is the right time to see a doctor according to your age-related fertility concerts, for example:
- Under 35: if you’ve tried for 12 months without success.
- Age 35–39: after 6 months of regular attempts.
- Age 40+: consider prompt evaluation before or as you start trying.
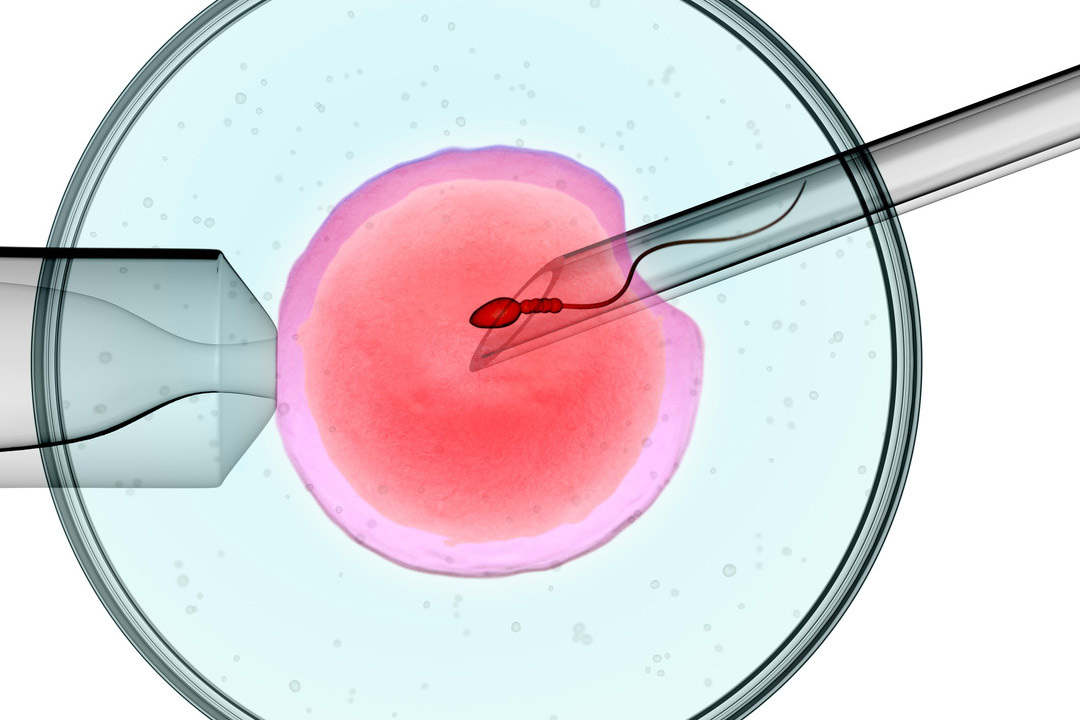
IVF at Advanced Age
IVF can still lead to a healthy birth in the late 30s and 40s, but success with your own eggs drops as age rises; donor eggs can restore much of the age-related loss in egg quality.
- Chances: Live-birth rates per transfer are highest before 35, fall through 38–40, and are low in the mid-40s with their own eggs. Donor-egg IVF generally has much higher success across ages.
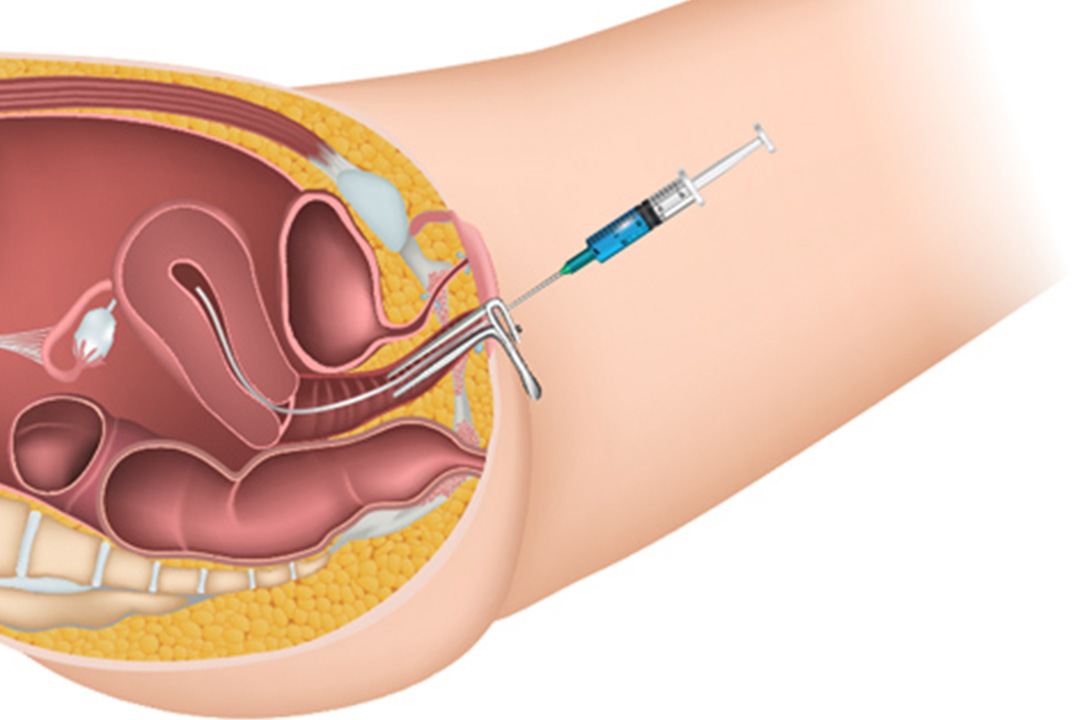
- What speeds things up: Do baseline tests early (AMH, antral follicle count, uterine scan, semen analysis) and plan for more than one cycle if using your own eggs. Some choose embryo banking to increase the chance of finding a chromosomally normal embryo.
- PGT-A (chromosome screening): May help avoid transferring embryos with aneuploidy in selected patients who produce multiple embryos; it doesn’t guarantee a live birth.
- Transfer strategy: Single-embryo transfer is usually safer and doesn’t reduce overall chances across multiple transfers.
- Costs (India): Expect roughly ₹1.2–3.0 lakhper IVF cycle in many private settings (more with add-ons like ICSI/PGT-A or donor eggs).
Tips for Healthy Pregnancy
Despite the age range, there are some common tips you can follow to ensure a healthy pregnancy, for example:
- Schedule a pre-pregnancy check-up. Review health conditions, medicines, vaccines, and start folic acid (≥400 mcg/day) ideally at least one month before conception.
- Quit smoking and avoid alcohol. Both reduce fertility and raise pregnancy risks; stopping beforehand is best.
- Manage weight and chronic conditions. Aim for a healthy BMI and optimize conditions like diabetes or hypertension before conceiving.
- Keep caffeine moderate. Guidance supports ≤200 mg/day during pregnancy.
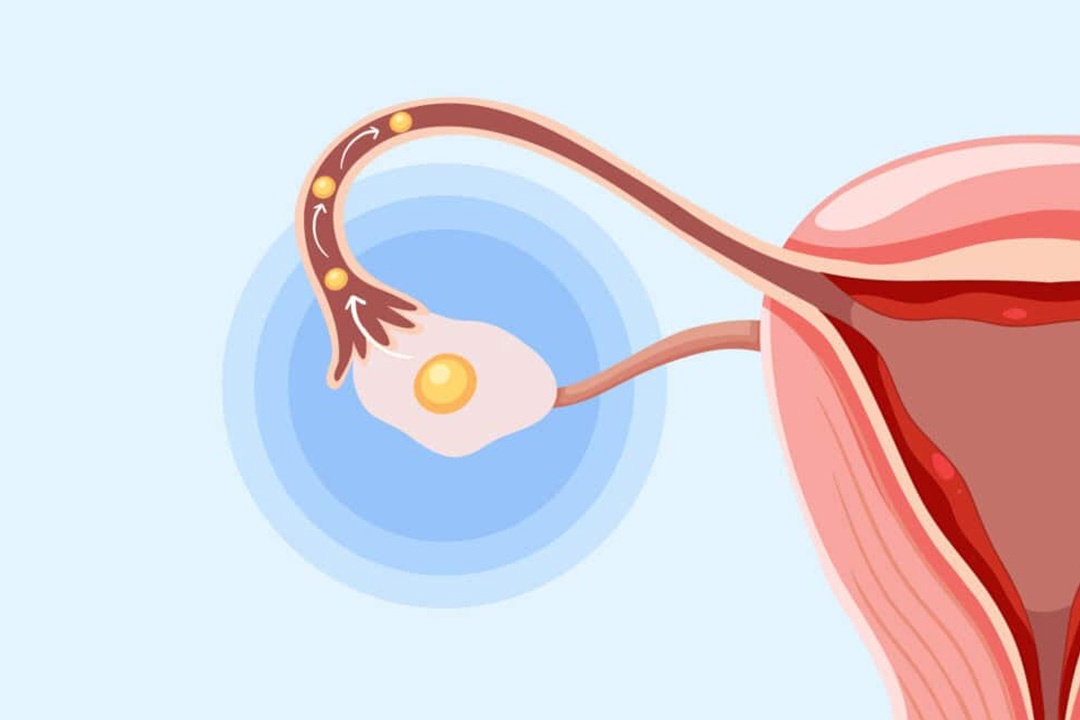
- Time intercourse during the fertile window. Likelihood of conception is highest in the few days before and the day of ovulation.
Age and Genetic Screening
As maternal age increases, the chance of chromosomal differences (like trisomy 21) rises. Today, non-invasive prenatal testing (NIPT) and diagnostic options can assess risk early in pregnancy; counseling helps choose the right approach for you.
Note that although risk rises with age, most babies with Down syndrome are born to younger mothers because more births occur in those age groups.
Frequently Asked Questions
Should I freeze my eggs “just in case”?
Egg freezing can preserve the current quality of eggs, not reverse aging. It may make sense if you need to defer childbearing for medical or personal reasons, but it’s not a guarantee of a future live birth. A consultation can help you understand likely egg numbers to freeze at your age and realistic outcomes.
What about miscarriage risk as I get older?
Miscarriage becomes more common with age, largely due to chromosomal changes in eggs. Estimates suggest early pregnancy loss is ~9–17% in the 20s and rises from about 20% at 35 to around 40% by 40; personalized risk varies by health and history.
Do men’s ages matter during conception too?
Yes, male fertility also declines with age, though more gradually. Sperm quality and some pregnancy outcomes can be affected, so both partners may benefit from evaluation when a couple faces difficulty conceiving.
Conclusion
From the first period to menopause, pregnancy is biologically possible, but the probability and risk profile change with age. Many people achieve healthy pregnancies in their 20s and 30s; many also do so in their late 30s and 40s with appropriate care.
If you’re planning ahead, think of age as one factor among many alongside your health, your support system, and your personal readiness. When in doubt, schedule a preconception visit and discuss a plan that fits your goals and timeline.
About Us
AKsigen IVF is a premier center for advanced fertility treatments, with renowned fertility experts on our team. Specializing in IVF, ICSI, egg freezing, and other cutting-edge reproductive technologies, AKsigen IVF is committed to helping couples achieve their dream of parenthood. With personalized care and a patient-first approach, AKsigen IVF provides comprehensive fertility solutions under one roof.