What is Retrograde Ejaculation?: Meaning, Causes, and Treatment Options
Usually, orgasm ends with semen leaving the penis in a visible stream. In some men, however, climax feels normal but little or no semen comes out. That experience can be confusing and even worrying, especially if you’re planning a pregnancy.
Retrograde ejaculation is the medical term for this pattern. It describes a situation where semen flows backward into the bladder during orgasm instead of exiting the body through the urethra. The sensation of climax is typically unchanged, but the “visible part” of ejaculation is reduced or absent.
This article explains what’s going on, why it happens, who’s at risk, how clinicians confirm the diagnosis, and what you can do if you’re trying to conceive.
What exactly is Retrograde Ejaculation?
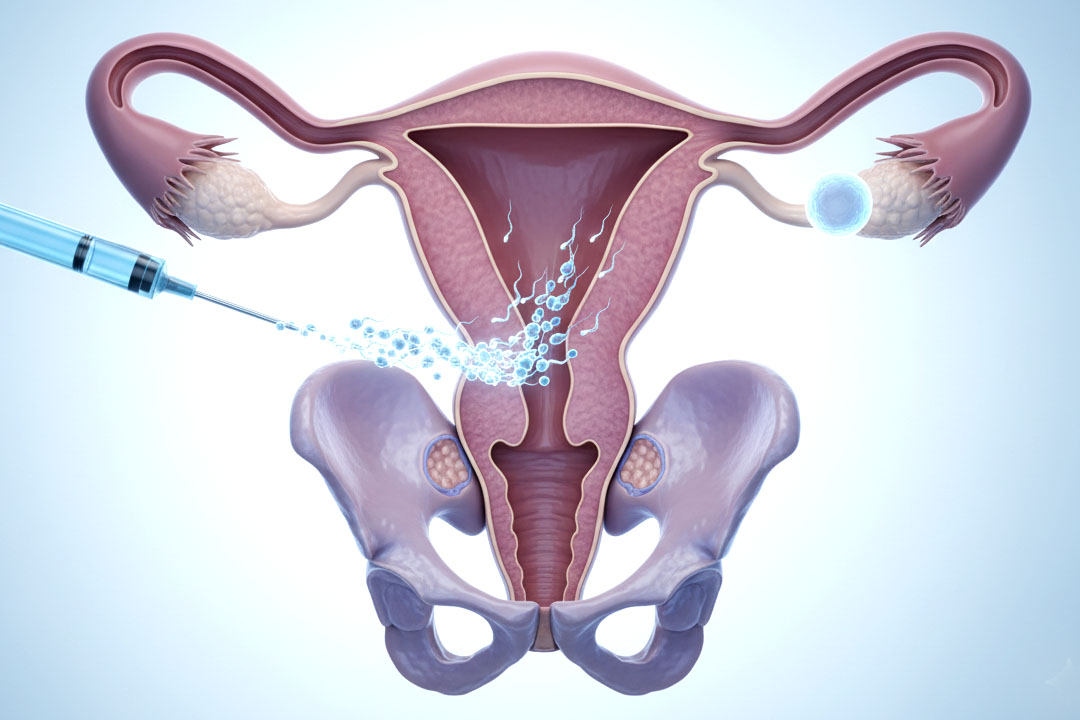
It means semen travels the wrong way which is back into the bladder when you orgasm, so little or none appears outside. Under usual circumstances, a ring of smooth muscle at the bladder neck (often called the internal sphincter) shuts tightly at orgasm. That closure acts like a one-way valve, directing semen forward through the urethra.
In retrograde ejaculation, that muscle doesn’t close properly. The path into the bladder stays open, and semen follows the path of least resistance into urine. You’ll often notice a “dry” or very low-volume ejaculation and then slightly cloudy urine after sex because semen mixes with urine and leaves your body when you urinate.
How Ejaculation Normally Works and Why Does Direction Matters?
Semen is propelled by coordinated contractions of the prostate, seminal vesicles, vas deferens, and pelvic floor muscles. At the same moment, the bladder neck closes to keep semen from going the wrong way. This tight timing forward pump plus closed “back door” is what produces a visible ejaculation. When the bladder neck fails to close, the forward pump still happens, the orgasm still feels like an orgasm, but semen is diverted into the bladder.
Why does Retrograde Ejaculation Happen?
Anything that weakens, disables, or bypasses the bladder-neck “valve” can cause it. Common reasons include:
- Surgery on the prostate or bladder neck (e.g., TURP). Removing or reshaping tissue at the bladder outlet often disrupts the closing mechanism. Reported rates of retrograde ejaculation after standard TURP range roughly 50%–75%, depending on technique and study.
- Nerve damage from conditions like diabetes, multiple sclerosis, or spinal cord injury. Autonomic nerve injury impairs the reflex closure of the bladder neck, so semen more easily refluxes backward.
- Medications that relax the bladder neck or alter ejaculation. Alpha-blockers for urinary symptoms, some antidepressants, and other adrenergic-acting drugs can reduce sphincter tone and lead to “dry” climax.
- Urethral or pelvic procedures. Operations on the urethra or rectum can change anatomy or nerve signaling in ways that disturb the normal direction of flow.
What does Retrograde Ejaculation feel like?
Orgasm usually feels normal, but there’s little or no semen, and urine may look cloudy afterward. Most men report no pain and no change in erection or climax intensity. The main difference is low-volume or “dry” ejaculation and the observation that the first urine after sex is hazy because it contains semen.
Can Retrograde Ejaculation cause Sexual Dysfunction?
It typically doesn’t impair erections or pleasure, but it can affect confidence or satisfaction. The condition by itself doesn’t damage sexual function. Stress about the change is common, particularly during family-building, but the physical ability to have sex and orgasm remains intact. Counseling or reassurance often helps if worry is reducing enjoyment.
Retrograde Ejaculation & Diabetes
Diabetic autonomic neuropathy can prevent bladder-neck closure at orgasm and that leads to semen refluxes into the bladder (“dry” or very low-volume ejaculation).
Who’s at risk: Longer diabetes duration, poor glycemic control, coexisting neuropathy; alpha-blockers or certain antidepressants can worsen it.
Management: Optimize diabetes control + review meds; consider bladder-neck–tightening agents and if needed, retrieve sperm from post-ejaculatory urine for IUI/IVF.
How do Doctors Diagnose Retrograde Ejaculation?
It is diagnosed by checking semen volume and looking for sperm in urine collected right after orgasm. A typical evaluation includes your symptom history, a physical exam, and one or both of the following:
- Low semen volume on repeated samples. Persistently tiny volumes suggest semen may be going elsewhere.
- Post-ejaculatory urinalysis. You empty your bladder, climax (by masturbation), then provide a urine sample immediately. If lab staff find sperm (and often semen markers like fructose) in that sample, it confirms that semen flowed into the bladder.
- If there’s a “dry orgasm” without sperm in urine, clinicians look for other causes (for example, very low semen production after pelvic radiation or gland damage).
Is Retrograde Ejaculation Harmful?
It isn’t dangerous, but it can make natural conception difficult. Retrograde ejaculation doesn’t injure the bladder or prostate, and your body safely passes semen with urine. The main medical implication is infertility, because very little semen reaches the vagina during intercourse.
What are the treatment options for Retrograde Ejaculation?
Many men don’t need treatment; if you’re trying to conceive, options include medication or assisted reproductive techniques.
- If you’re comfortable and not trying for a pregnancy, no treatment is necessary. When a medication is the trigger, clinicians often switch to an alternative and reassess, sometimes that alone restores forward ejaculation.
- When pregnancy is a goal, doctors may try “sympathomimetic” or related agents that increase tone at the bladder neck.
- If medication doesn’t help, fertility teams can recover sperm from urine collected immediately after orgasm. Preparing the bladder beforehand (alkalinizing the urine, adjusting timing, and using lab processing to isolate motile sperm) increases the chances of obtaining usable sperm for intrauterine insemination (IUI) or IVF/ICSI.
- When urine-based recovery fails or there’s also a problem with sperm production, specialists may consider procedures such as microsurgical testicular sperm extraction (micro-TESE) combined with IVF/ICSI. This is usually reserved for complex cases.
Imipramine for Retrograde Ejaculation
Tricyclic with noradrenergic action increases sympathetic tone at the bladder neck, promoting forward ejaculation. It can be used if fertility is desired and no reversible medication cause; often tried alone or combined with pseudoephedrine for higher success.
Expected outcomes: Restoration of antegrade ejaculation in a subset; combination therapy can improve rates vs single agents.
Safety notes: Monitor BP/HR; watch for anticholinergic effects, sedation, QT risk, and drug interactions, avoid in contraindicated cardiac/ophthalmic/urinary conditions.
If no response, proceed to post-ejaculatory urine sperm retrieval for IUI, or escalate to IVF/ICSI; consider alternative agents (e.g., pseudoephedrine, midodrine).
Can Retrograde Ejaculation be prevented?
Not always, but some choices may reduce risk around prostate treatment. Before any prostate or bladder-neck surgery, discuss ejaculation outcomes with your urologist. Conventional TURP has high rates of retrograde ejaculation, while newer minimally invasive options (such as prostatic urethral lift or water-vapor therapy/Rezūm) aim to relieve urinary symptoms while better preserving ejaculatory function in appropriate candidates.
Procedure selection depends on prostate size, anatomy, and goals; the priority is always symptom relief and safety, but preserving ejaculation is now part of shared decision-making.
If you’re starting a medication for urinary symptoms or depression and ejaculation is a priority, ask about alternatives with a lower likelihood of this side effect. When surgery is planned and you hope for children later, sperm banking before the procedure is a practical safeguard.
Frequently Asked Questions
Is IVF for me if I have retrograde ejaculation?
If medication or urine-sperm retrieval doesn’t yield enough motile sperm for IUI, IVF often with ICSI is a logical next step regardless of age. The decision depends more on sperm availability/quality and your partner’s fertility profile. A reproductive specialist will usually try the least invasive successful option first (e.g., IUI using urine-recovered sperm) before moving to IVF/ICSI.
Is there a quick way to tell if I have retrograde ejaculation?
A post-ejaculatory urine test is the standard confirmatory step. After urinating and then climaxing, you give a urine sample; finding sperm (and semen markers) in that sample supports the diagnosis.
Can pelvic floor (Kegel) exercises fix retrograde ejaculation?
They can improve urinary control and sexual confidence, but they don’t force semen forward if the bladder neck stays open. The issue is the smooth muscle “valve,” not pelvic floor strength.
If mine started after prostate surgery, will it go away?
Often it’s long-lasting after procedures that remove or disrupt the bladder neck, such as standard TURP. Some technique variations and newer minimally invasive options aim to preserve ejaculation, but once the bladder-neck mechanism is altered, reversal is uncommon.
What medications can help and are they safe?
Pseudoephedrine, imipramine, or midodrine may be tried to tighten the bladder neck, but they’re not right for everyone. These drugs can raise blood pressure/heart rate and may interact with other medicines, so they should be used under clinical guidance.
If I pee out semen, is that unhealthy for the bladder?
No. It mixes with urine and is eliminated; there’s no evidence that this harms the bladder or kidneys. The main challenge is fertility, not safety.
Conclusion
Retrograde ejaculation can feel unsettling, but it’s usually harmless and very manageable once you know what’s going on. The main concern is fertility, and even there, you have practical paths forward: reviewing medications, trying targeted therapies that tighten the bladder neck, or using assisted options like post-ejaculatory urine sperm recovery, IUI, or IVF/ICSI when needed.
If your symptoms began after prostate or urethral surgery, the change may persist, yet support and solutions still exist. The most helpful next step is a straightforward evaluation to confirm the cause and tailor a plan that fits your goals.
About Us
AKsigen IVF is a premier center for advanced fertility treatments, with renowned fertility experts on our team. Specializing in IVF, ICSI, egg freezing, and other cutting-edge reproductive technologies, AKsigen IVF is committed to helping couples achieve their dream of parenthood. With personalized care and a patient-first approach, AKsigen IVF provides comprehensive fertility solutions under one roof.