Can IUI Be Successful After a Failed IVF Cycle?
When a much-hoped-for IVF cycle fails, it’s normal to feel stuck. You’ve invested time, emotion, and money and the idea of starting over can be daunting. Some couples are advised to go straight into another IVF attempt. Others look for another option.
That’s often where intrauterine insemination (IUI) enters the conversation. IUI is not a downgrade, it’s a different approach with a different risk–benefit balance. For the right candidates, it can be a sensible next step that keeps momentum without the intensity of a full IVF cycle.
This article explains when IUI after IVF makes sense, what shapes the odds, and how to make an informed decision that fits your medical picture and personal bandwidth.
What is IVF and IUI?
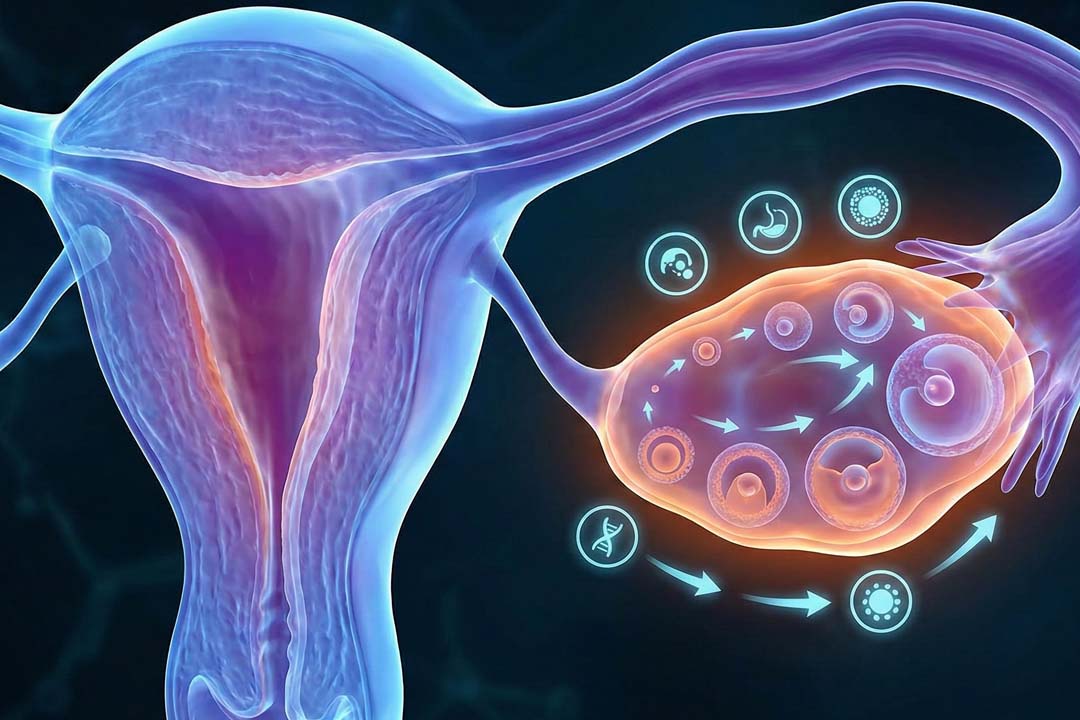
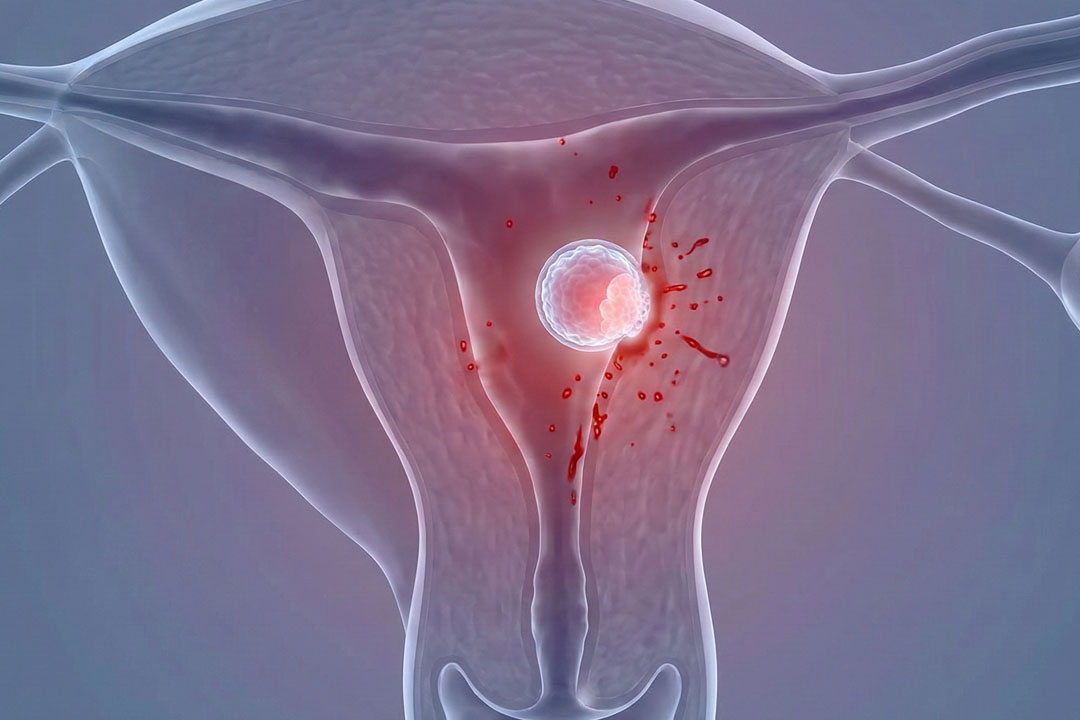
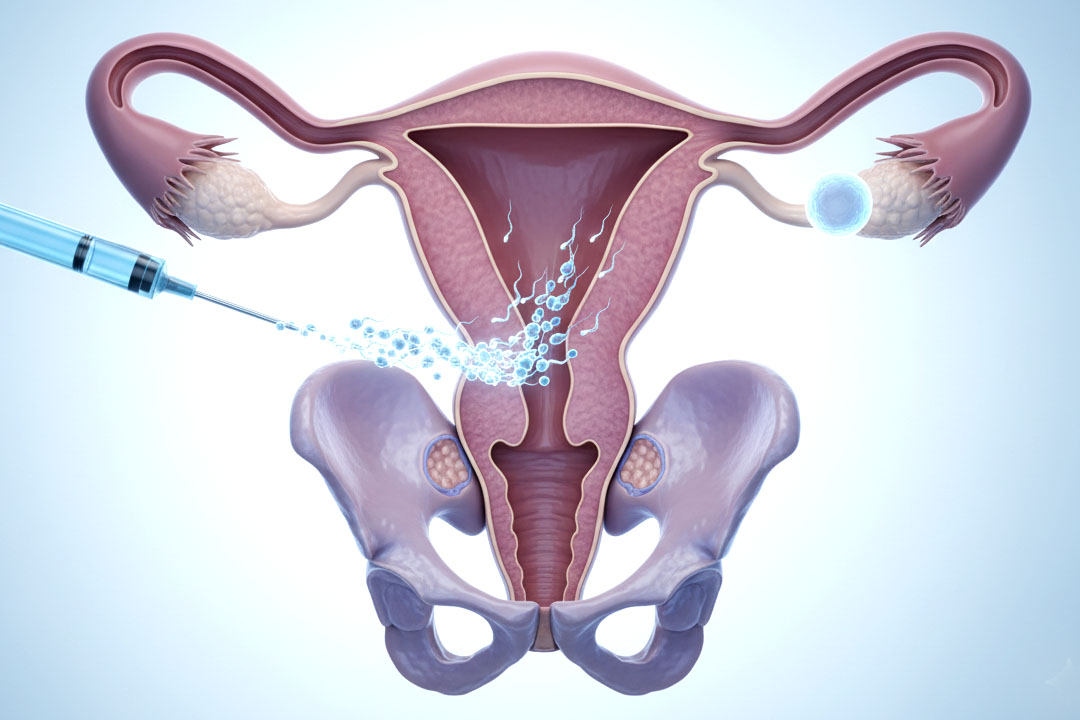
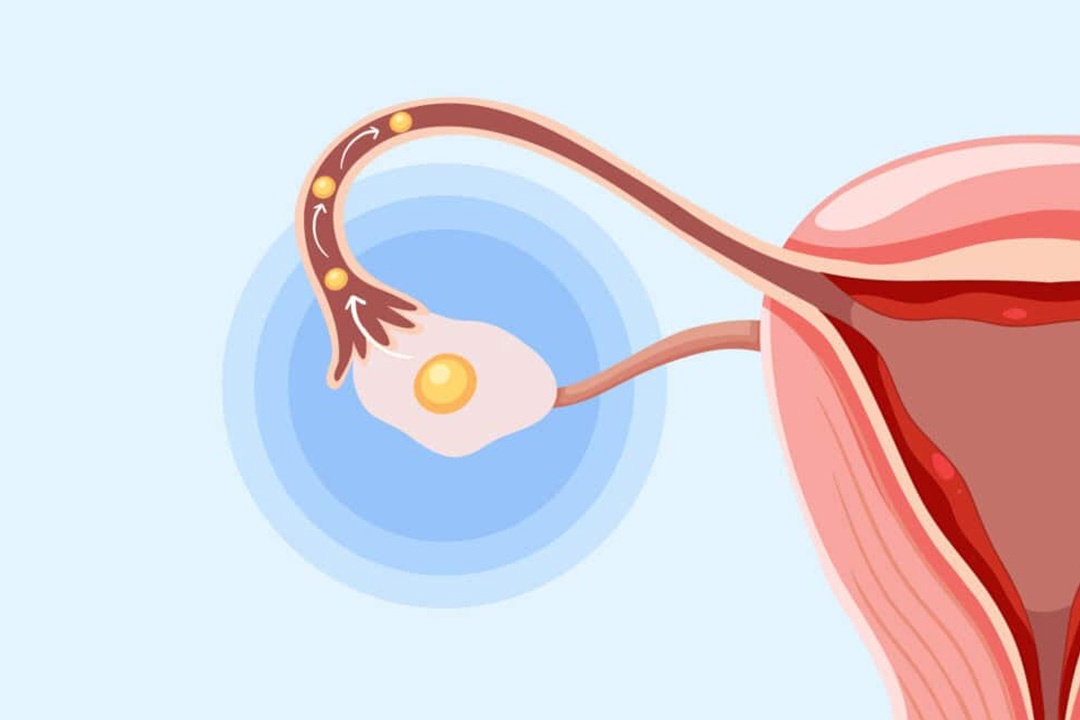
IUI places prepared sperm directly into the uterus around ovulation. It may be done in a natural cycle or with mild stimulation. The goal is to shorten the sperm’s journey and time the insemination precisely.
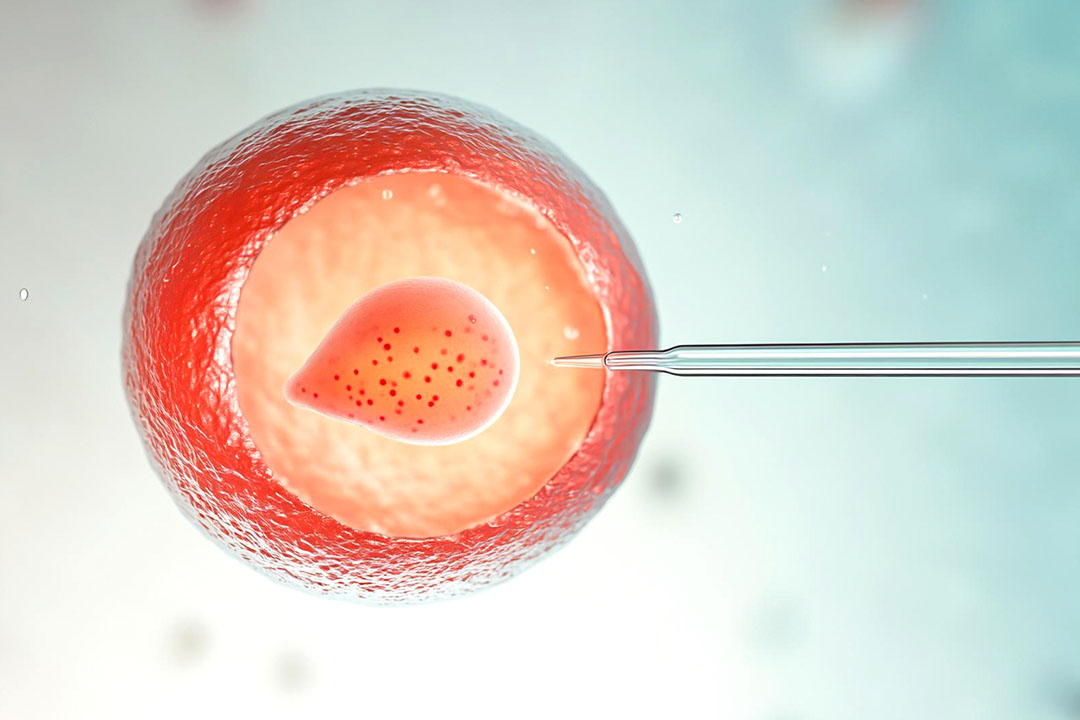
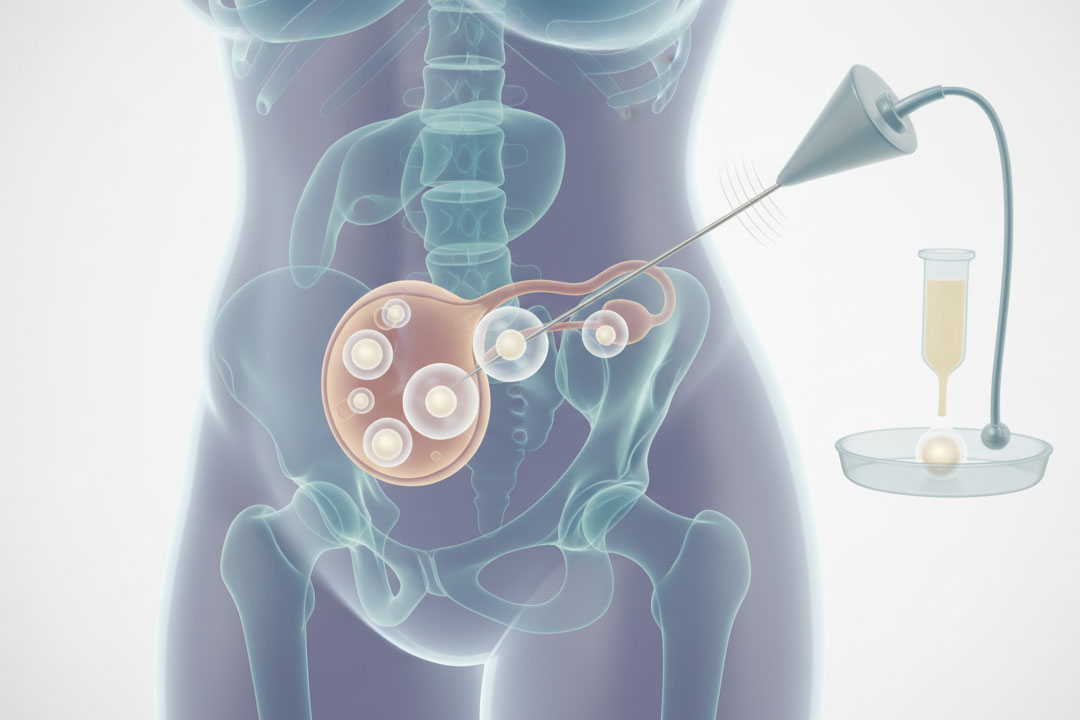
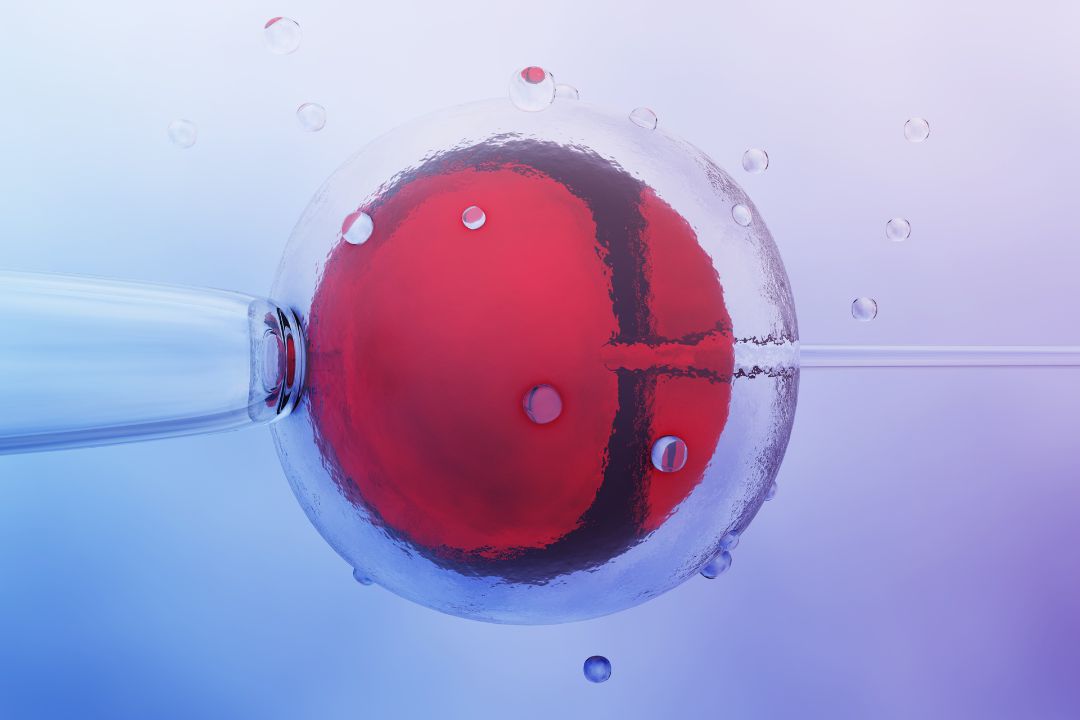
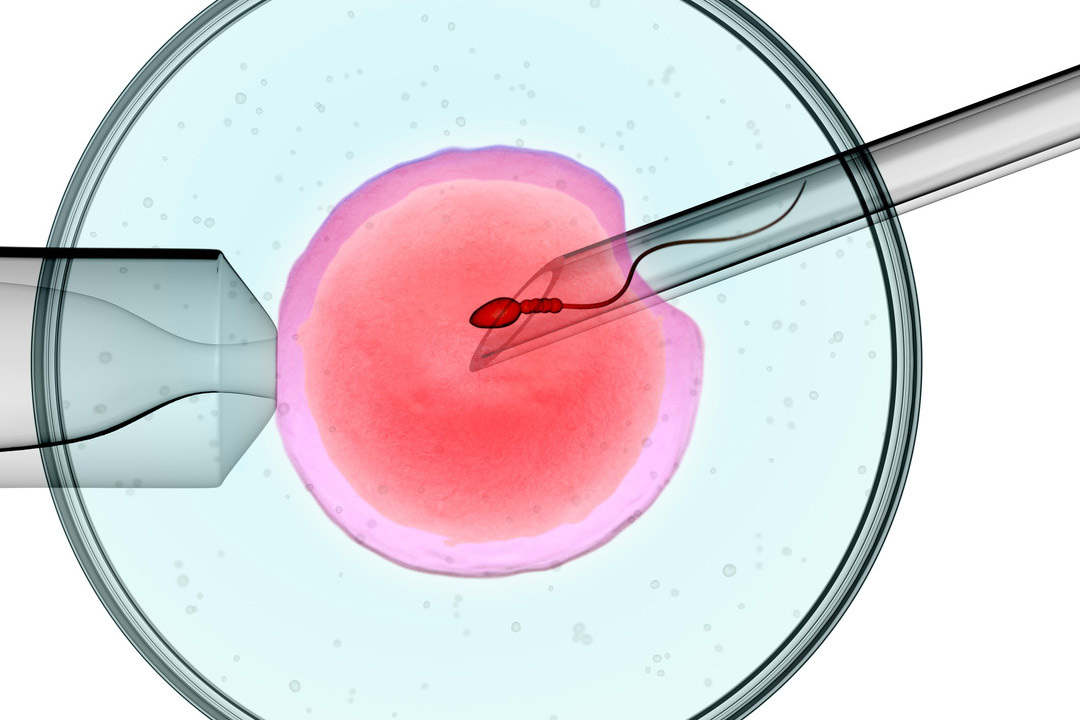
IVF stimulates the ovaries to grow multiple follicles, retrieves the eggs, fertilises them in the lab, and transfers an embryo back into the uterus. It involves more steps, more medicines, and higher costs, but it also has higher per-cycle success rates.
Key Points
- Complexity: IUI is a quick outpatient procedure; IVF involves stimulation, egg retrieval, and lab work.
- Cost: IUI is markedly less expensive.
- Medication load: IUI may need little or no injectables; IVF typically uses them.
- Success rates: IVF is generally higher; IUI can still work for selected cases.
Is IUI Worth Trying After a Failed IVF Cycle?
Often yes, if your diagnosis and test results point to a reasonable chance with less intervention. IUI may be worth considering when tubes are open, sperm parameters are workable, and the main issue is timing or mild subfertility. It’s also a sensible option for couples who prefer a break from the intensity of IVF while still moving forward. If previous IVF revealed useful clues (for example, that fertilisation was achieved and the uterine cavity looked healthy), your team might tailor an IUI plan around those insights.
Who Can Benefit the Most?
People with
unexplained infertility, mild male factor, cervical factor, mild endometriosis, or ovulatory issues that respond to gentle stimulation often see the best odds with IUI. Donor sperm IUI can be particularly effective when partner sperm parameters are borderline or when previous IVF raised concerns about sperm function.
Age matters too.
Under 35s typically have higher IUI success than older age groups, and some patients in their late thirties still do well if ovarian reserve is reassuring and tubes are open.
What Increases the Odds After IVF?
Several elements move the needle:
- Age: Egg quality tracks with age. Under 35 generally fares better; outcomes dip in the forties.
- Ovarian reserve: AMH, AFC, and prior response to stimulation help predict how well a lightly stimulated IUI cycle might go.
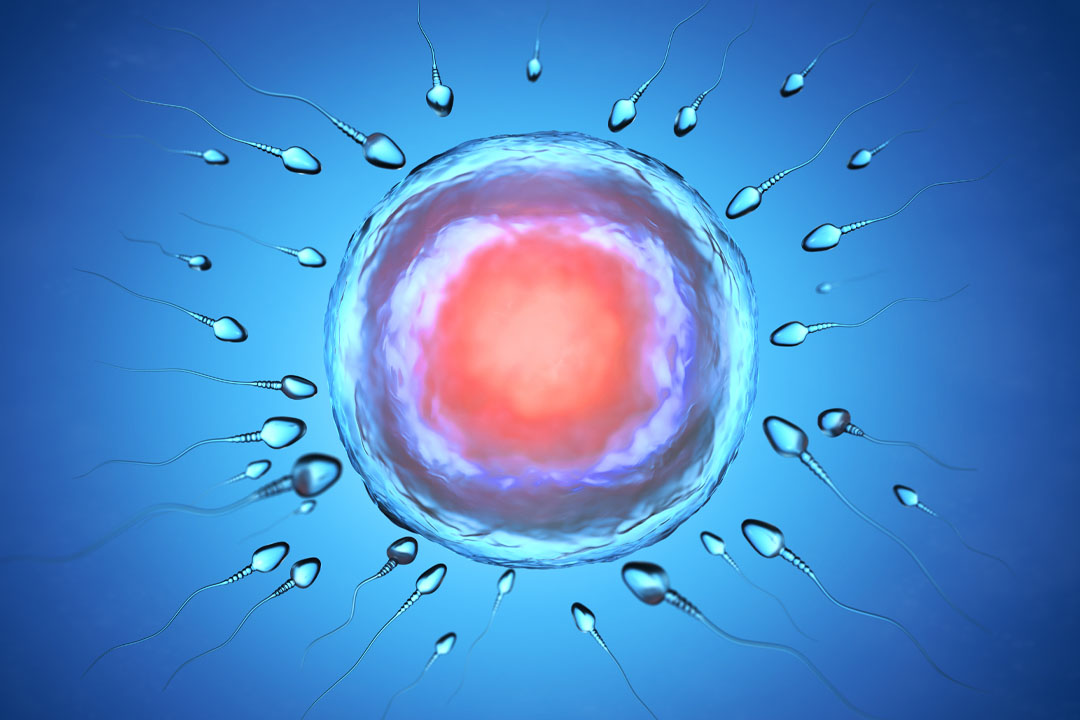
- Sperm quality: Total motile sperm count (TMSC) and morphology matter. Higher TMSC at insemination is linked to better results.
- Tubal status: At least one patent tube is essential.
- Uterine and endometrial health: Polyps, adhesions, or untreated fibroids can reduce chances and should be addressed.
- Timing: Insemination must line up closely with ovulation; a clinic with tight monitoring improves precision.
- Cycle protocol: Natural vs. stimulated IUI, the choice of oral agents vs. low-dose gonadotropins, and the use of a trigger shot can all influence success.
- Lifestyle and health factors: A healthy BMI, non-smoking, limited alcohol, good sleep, and stress management are associated with better semen parameters and ovulatory patterns, which indirectly improve IUI outcomes.
- Number of attempts: Some patients especially in their thirties see improved odds by the second or third IUI.
How Much Success Should You Realistically Expect?
Per-cycle pregnancy rates after IVF failure are generally modest with IUI often in the range of 5–15% with partner sperm and higher when donor sperm is used but the range is wide because diagnosis, age, and protocol vary.
In carefully chosen cases (younger age, good ovarian reserve, clear tubes, solid TMSC, well-timed insemination with appropriate ovulation induction), some clinics report 15–20% per cycle. That is still lower than IVF, but the lower cost and lighter physical toll make IUI an acceptable trade-off for many.
- Donor sperm IUI frequently outperforms partner-sperm IUI because donor samples are pre-screened and often show strong motility.
- Cycle one vs. cycles two and three: It’s common for the second or third attempt to yield better results, particularly in older groups where the first IUI may serve as a learning cycle for dose and timing.
How Many IUI Cycles are Reasonable to Try?
Two to three well-timed IUIs are a common ceiling before re-evaluating. If you’re under 35 with a good ovarian reserve and suitable diagnosis, trying up to three cycles can be reasonable. For late thirties and early forties, time matters more; many teams limit IUI to two cycles unless there’s a strong reason to continue. If you haven’t conceived by then, the probability of ongoing success with further IUI tends to fall, and moving back to IVF may be more time-efficient.
When is IUI Not the Right Choice?
IUI is unlikely to help when:
- Both tubes are blocked or severely damaged.
- Severe male factors are present (very low TMSC or morphology) or there are known sperm functional issues.
- Significant uterine pathology remains untreated.
- Advanced maternal age (typically 40+) is combined with low reserve; in these cases, IVF may offer a better path in the limited time available.
- Genetic testing of embryos is a priority because of known heritable conditions; that require IVF.
How soon after a failed IVF can you attempt IUI?
Many couples try within three to six months, which gives time for the body to reset and for your team to apply lessons from the IVF cycle (for example, how your hormones responded, whether luteal support is needed, or whether ovulation timing should be adjusted). Some start sooner if physically ready and emotionally comfortable; others choose a longer pause.
What Does an IUI cycle Look Like After IVF?
While specific plans vary, a typical pathway is:
- Baseline check (cycle day 2–3): Ultrasound and bloods to confirm a clean start.
- Ovulation strategy:
- Natural cycle if you ovulate regularly; or
- Oral stimulation (e.g., letrozole or clomiphene) to grow one or two follicles; or
- Low-dose gonadotropins when a stronger push is needed.
- Monitoring: One to three scans and occasional blood tests to track follicle growth and lining.
- Trigger and timing: A trigger shot may be used to schedule ovulation. Insemination is typically about 24–36 hours later.
- Semen preparation: The lab washes and concentrates motile sperm to maximize the TMSC used for IUI.
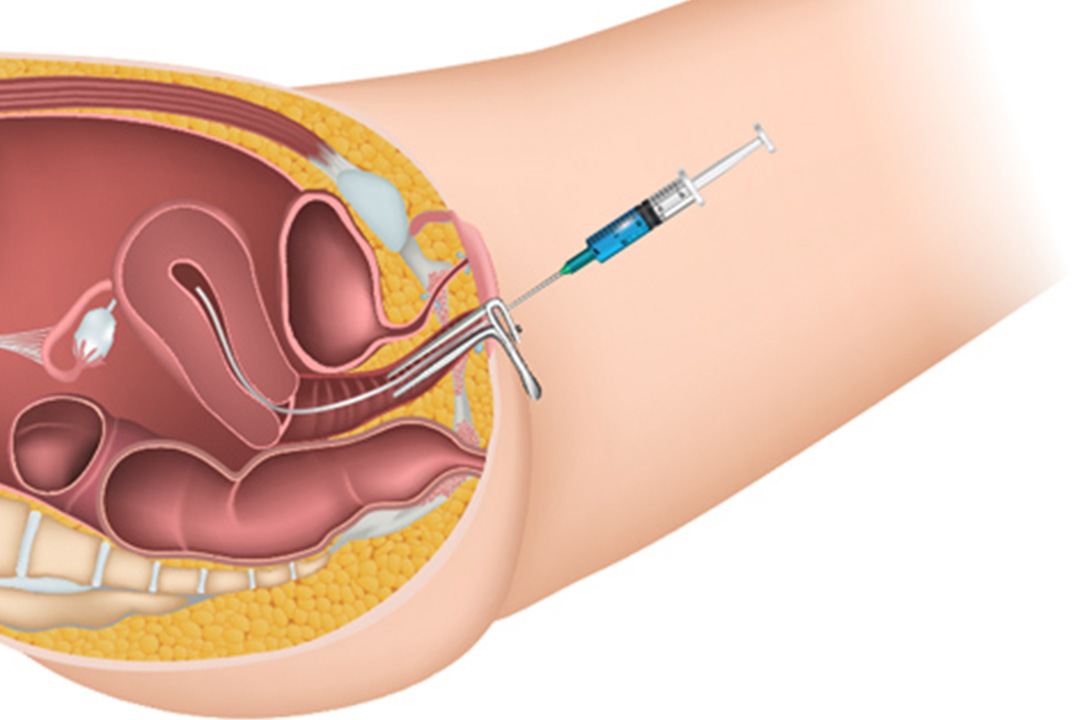
- The procedure: A fine catheter places the prepared sample into the uterus. It takes minutes and you can resume normal activity right after.
- Luteal support: Some protocols add progesterone for two weeks.
- Pregnancy test: Around 14 days after IUI.
Risks to Know
There are very few risks but it is important to keep them in mind:
- Lower success than IVF: Per-cycle rates are usually lower, so multiple attempts may be needed.
- Multiple pregnancy: The risk rises with stimulation (especially if several follicles develop). Careful dosing and cancellation criteria help manage this.
- Time cost: If age or reserve is a concern, time spent on IUI might reduce the window for IVF.
- Emotional wear: Even “lighter” treatments can be stressful; plan support and rest between cycles.
FAQs
Does BMI really affect IUI success?
Yes, both under- and overweight ranges can affect hormones, ovulation, and implantation. Aiming for a healthy BMI improves cycle predictability and is associated with better outcomes, particularly when stimulation is used.
What is a “good” total motile sperm count for IUI?
Higher is better, and labs generally prefer a solid TMSC after preparation. While pregnancies can occur at lower counts, chances improve as motile numbers rise. Your clinic will discuss whether your specific numbers are appropriate for IUI or whether IVF (or IVF with ICSI) makes more sense.
Can IUI work after IVF if my ovarian reserve is borderline?
It can, but the window is tighter and per-cycle odds are lower. If time is a concern or reserve is low, you and your doctor may prioritise a swift return to IVF so you don’t lose valuable months.
Is natural-cycle IUI as good as stimulated IUI?
It depends on the reason for infertility. Natural cycles avoid the risk of multiples and may suit regular ovulators. Mild stimulation can raise the chance of at least one mature follicle and can help clinics schedule insemination more reliably.
Will stimulation increase the chance of twins?
It can. The risk correlates with the number of mature follicles. Careful dosing, monitoring, and cycle cancellation policies are designed to keep this risk low.
If IVF success rates are higher, why try IUI at all?
Because success isn’t the only metric; burden matters too. IUI is quicker, cheaper, and less invasive. For suitable candidates, a short IUI trial is a reasonable way to keep moving without the full weight of another IVF round.
Does donor sperm really change the odds?
Often yes. Donor samples are typically high quality, and donor IUI is commonly associated with better per-cycle success than partner-sperm IUI when partner parameters are borderline.
What if our first IUI fails?
Don’t be discouraged by a single attempt. Many conceive on the second or third try. If you set a stop-rule in advance, the next step, whether another IUI or a return to IVF will feel more straightforward.
Conclusion
IUI can be successful after a failed IVF cycle, but it thrives on the right conditions: open tubes, workable sperm counts, a clear and timely protocol, and (ideally) younger age with solid ovarian reserve. Per-cycle chances are generally lower than IVF, yet the lighter physical and financial load makes IUI a sensible bridge for many.
If you decide to try, consider two to three carefully monitored cycles, keep lifestyle and health factors tuned up, and agree on when to pivot if pregnancy hasn’t happened. Most importantly, choose the path that fits your diagnosis and your capacity—your plan should support both your medical goals and your well-being.
About Us
AKsigen IVF is a premier center for advanced fertility treatments, with renowned fertility experts on our team. Specializing in IVF, ICSI, egg freezing, and other cutting-edge reproductive technologies, AKsigen IVF is committed to helping couples achieve their dream of parenthood. With personalized care and a patient-first approach, AKsigen IVF provides comprehensive fertility solutions under one roof.