Which Size of Fibroid is Dangerous?: Symptoms & Treatment Options
Fibroids (uterine leiomyomas) are very common, usually non-cancerous growths of the uterus. Many people have them without ever knowing; others have symptoms such as heavy periods, pelvic pressure, or frequent urination.
Size often becomes the first worry after an ultrasound report but size alone rarely tells the whole story. Where a fibroid sits (inside the cavity vs. in the wall vs. on the outside), how many there are, how fast they’re growing, and whether you want future pregnancy all change what “risky” means for you.
In short: a small fibroid in the wrong place can cause big trouble, while a larger one in a less sensitive spot might be quiet for years. This guide explains how size interacts with symptoms, fertility, and pregnancy risks and when to consider treatment.
Is there a “dangerous” fibroid size?
There isn’t a single cut-off that is always dangerous; risk depends on size + number + location + symptoms + goals (e.g., fertility). That said, evidence and guidelines flag a few useful thresholds:
- Greater than 3 cm: if you’re symptomatic, guidelines advise specialist review and note that some medicines work less well as fibroids get “substantially” larger than 3 cm.
- Greater than 5 cm: larger fibroids are more likely to cause pressure symptoms; in pregnancy, fibroids above ~5 cm are linked to more pain (degeneration) and certain obstetric risks.
- Greater than 10 cm: very large fibroids carry higher risks of maternal complications and preterm birth in pregnancy.
How Fibroids Grow (and Why Location Matters More Than People Think)
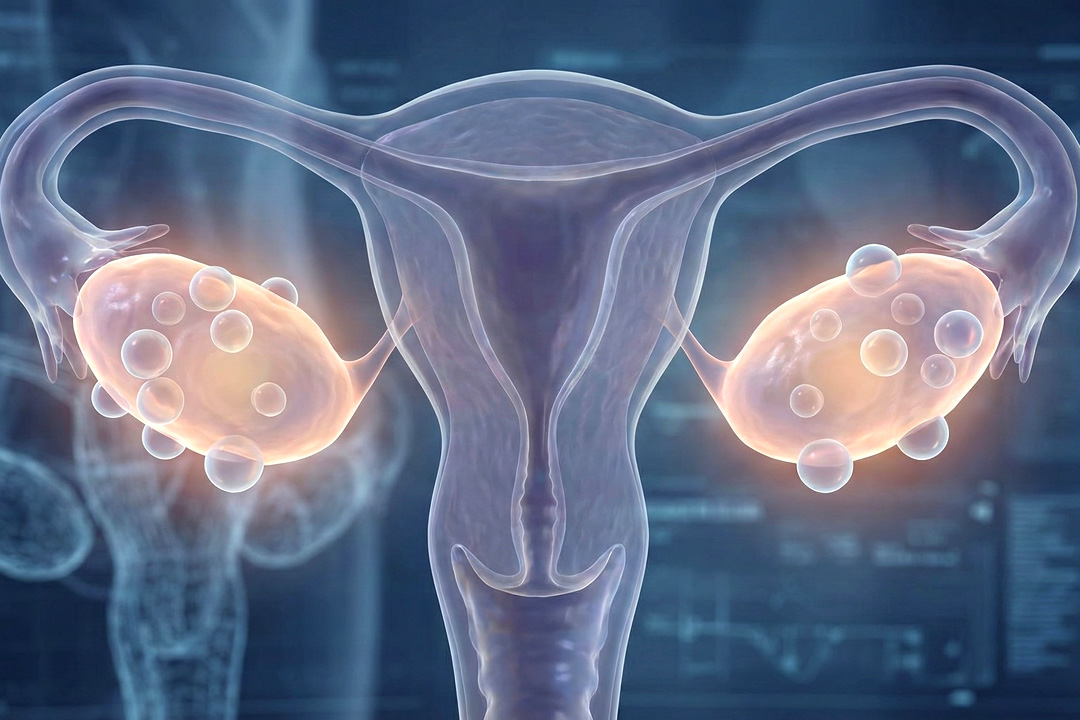
Fibroids arise from the uterine muscle and can be intramural (in the wall), submucosal (jutting into the uterine cavity), subserosal (bulging outward), or pedunculated (on a stalk). Submucosal fibroids, even when small, can trigger heavy bleeding and reduce fertility because they distort the cavity.
Intramural lesions may reduce implantation if they’re big enough to deform the cavity, while subserosal fibroids mostly cause “bulk” pressure. Some fibroids stay stable for years; others enlarge under hormonal influence, often shrinking after menopause. During pregnancy they may enlarge (especially early), and then often regress postpartum.
Which Fibroid Size is “Dangerous” in Pregnancy?
Risk rises with size. Fibroids >5 cm are linked with more pain from degeneration and certain obstetric issues; ≥10 cm fibroids show higher odds of maternal morbidity and earlier preterm birth in recent studies. Even so, many pregnancies with fibroids end well, and large fibroids are not an automatic reason to avoid a trial of labour.
Even 1–2 cm submucosal fibroids can cause significant bleeding or reduce the chance of implantation and live birth; removing the lesion hysteroscopically often improves outcomes.
How Fibroids are Diagnosed and Tracked
Pelvic exam + ultrasound are first-line; MRI helps map number, size, and location before procedures (or if ultrasound is limited) and in pregnancy complications. For heavy menstrual bleeding, guidelines advise specialist assessment once fibroids are bigger than 3 cm and note that medications may be less effective as size increases.
Is Rapid Growth a Red Flag for Cancer?
Cancer is rare, and there’s no reliable pre-op test that distinguishes a benign fibroid from a sarcoma. Estimates of unsuspected leiomyosarcoma at fibroid surgery range from roughly 1 in 570 or 1 in 8,300 depending on study design. Growth alone is not a reliable predictor, but any concerning change should prompt specialist evaluation.
Types of Fibroids Treatments
Different types of Fibroids require different types of treatment procedures, for example:
- Submucosal fibroids causing heavy bleeding/infertility. Hysteroscopic myomectomy (through the cervix) is first-line and fertility-sparing.
- Intramural or subserosal fibroids with bulk symptoms or cavity distortion. Laparoscopic/open myomectomy can remove fibroids and preserve the uterus.
- Uterine artery embolization (UAE/UFE) reduces blood flow to fibroids, shrinking them and improving bleeding/pressure. It is useful for multiple or larger fibroids if future pregnancy is not the immediate goal.
- Radiofrequency ablation (RFA) (select centres) treats smaller fibroids with heat; MR-guided focused ultrasound may help selected cases. Availability varies and candidacy depends on size, number, and location.
- Hysterectomy cures fibroids by removing the uterus. It is best reserved for severe, refractory symptoms when family completion is certain.
Fertility and IVF: Does Size Matter Here?
It depends upon the location. Submucosal fibroids and intramural fibroids that distort the cavity are consistently linked to lower fertility and higher miscarriage risk; removing them can improve outcomes. The impact of non–cavity-distorting intramural fibroids is debated, but studies suggest decreased IVF live-birth rates once sizes reach ~2–6 cm, and outcomes worsen above ~4 cm.
Will a 3–4 cm Intramural Fibroid Affect IVF?
It can, especially if it deforms the cavity; many clinics consider removal when an intramural fibroid approaches 4 cm and/or the cavity is indented, to optimize implantation. Decisions are individualized after imaging (saline sonogram or MRI) and discussion of prior IVF outcomes.
Pregnancy with Fibroids: Planning by Size and Site
Pain (“red degeneration”) is more likely with fibroids >5 cm and in the 2nd–3rd trimester; it’s typically managed conservatively (rest, acetaminophen, hydration) after ruling out other causes.
Malpresentation, labour dystocia, postpartum haemorrhage, preterm birth, especially when the largest fibroid is >e;10 cm or when multiple large fibroids are present. Most pregnancies still end well.
Plan extra surveillance if fibroids are >5 cm, submucosal, low-lying near the cervix, or numerous; mode of delivery is based on obstetric indications, not fibroid size alone.
Frequently Asked Questions
Is a 3 cm fibroid dangerous?
Usually no, especially if it sits on the outer surface (subserosal) and you have no symptoms. But a 3 cm submucosal fibroid can cause heavy bleeding or affect fertility because it distorts the uterine cavity.
Can a fibroid shrink on its own?
Yes. Many fibroids shrink after menopause, and some change size during and after pregnancy. Medical therapies can temporarily shrink them; procedures offer more definitive size reduction. Do I need surgery just because a fibroid is big? Not automatically. Surgery is considered for severe bleeding/anemia, bulk symptoms, cavity distortion, unclear diagnosis, rapid enlargement, or when fibroid size complicates pregnancy plans.
Will a 4–5 cm intramural fibroid affect IVF?
It might, especially if it indents the cavity. Many centres consider removing intramural fibroids around this size to improve implantation, but the decision is personalized.
Are medications enough for large fibroids?
Medicines can control bleeding and pain, but the effect on volume is limited and often temporary. Guidelines also support oral GnRH antagonist combinations for moderate–severe symptoms, with time limits for bone health. For persistent bulk symptoms, UAE/UFE or myomectomy are typical next steps.
Can pedunculated fibroids twist (torsion)?
Rarely, a fibroid on a stalk can twist and cut off its blood supply, causing sudden severe pain that needs urgent assessment.
Conclusion
“Dangerous” isn’t a single number, it’s the overall picture. A 2 cm submucosal fibroid that soaks your pads is more concerning than a quiet 6 cm subserosal one; a 10 cm intramural fibroid in someone planning pregnancy will be managed differently than in someone nearing menopause. If your report mentions fibroids, focus on how you feel, your blood count, where they sit, and what you want for future fertility.
About Us
AKsigen IVF is a premier center for advanced fertility treatments, with renowned fertility experts on our team. Specializing in IVF, ICSI, egg freezing, and other cutting-edge reproductive technologies, AKsigen IVF is committed to helping couples achieve their dream of parenthood. With personalized care and a patient-first approach, AKsigen IVF provides comprehensive fertility solutions under one roof.