Difference Between Laparoscopy and Hysteroscopy
Female pelvic health is complex, and many problems start inside the pelvis where routine external exams can’t see enough. That’s why minimally invasive tools are so widely used. Two of the most common are laparoscopy and hysteroscopy.
Both can diagnose issues and often treat them in the same sitting, but they look at different parts of the reproductive system, are done through different routes, and answer different clinical questions.
If you or someone you love is being evaluated for pain, irregular bleeding, miscarriages, or infertility, understanding how these procedures differ makes decisions less stressful and helps you prepare for what recovery is like.
This guide explains each method in, compares them side-by-side, and closes with FAQs people genuinely search before consenting to a procedure.
Main Differences Between Laparoscopy and Hysteroscopy
| Feature | Hysteroscopy | Laparoscopy |
|---|
| What it looks at | The inside of the uterus (uterine cavity and its lining). | The outside of the uterus, ovaries, fallopian tubes, and other pelvic organs |
| Access | Through the vagina and cervix; no abdominal cuts | Through small cuts on the abdomen with a camera and instruments. |
| How space is created | The uterine cavity is gently distended with fluid (usually saline) | The abdominal cavity is inflated with carbon dioxide (CO₂) to make room to see and work |
| Usual setting | Often outpatient/office for diagnostic or minor operative work; day-care possible. | Operating room; day-care in many cases. |
| Typical anesthesia | Local, oral/IV analgesia or light sedation; sometimes general anesthesia. | General anesthesia is standard. |
| Common reasons | Abnormal bleeding, suspected polyps/fibroids inside the cavity, adhesions, septum, recurrent miscarriage, infertility work-up. | Endometriosis, adhesions, ovarian cysts, fibroids on the outside of the uterus, blocked tubes, pelvic pain, ectopic pregnancy. |
| Cycle timing (if not urgent) | Best just after a period (follicular phase) for a clear view. | Often scheduled soon after menstruation during infertility evaluation. |
| Recovery | Same-day return to light activity; mild cramps/spotting for 1–2 days | 2–7 days to feel normal; shoulder tip pain or bloating is common for 24–48 hours. |
| Main risks (uncommon) | Uterine perforation, bleeding, infection, fluid overload (rare). | Injury to bowel, bladder, blood vessels; bleeding, infection, anesthesia risks. |
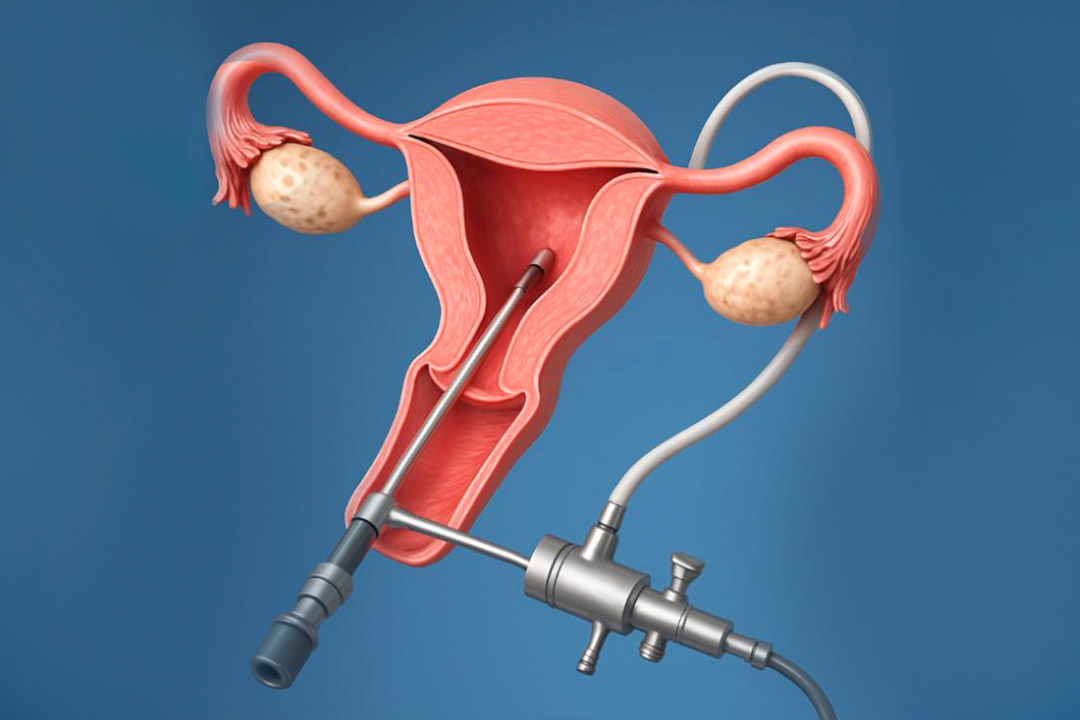
Hysteroscopy: Step by Step
A scope goes through the cervix; saline opens the cavity; the doctor looks and, if needed, treats small problems right away.
After consent, you lie on a gynecologic table. The cervix may be dilated a little (especially for operative cases). A slim hysteroscope is inserted through the cervix. Saline flows in to expand the space, giving a clear, magnified view of the lining, tubal openings, and cavity shape. If a polyp, small intracavitary fibroid, or scar is seen, tiny instruments passed through the scope can remove it.
Many diagnostic hysteroscopies are done without general anesthesia while operative ones may use deeper anesthesia depending on complexity and patient comfort. Light cramping and minimal spotting are common for a day or two.
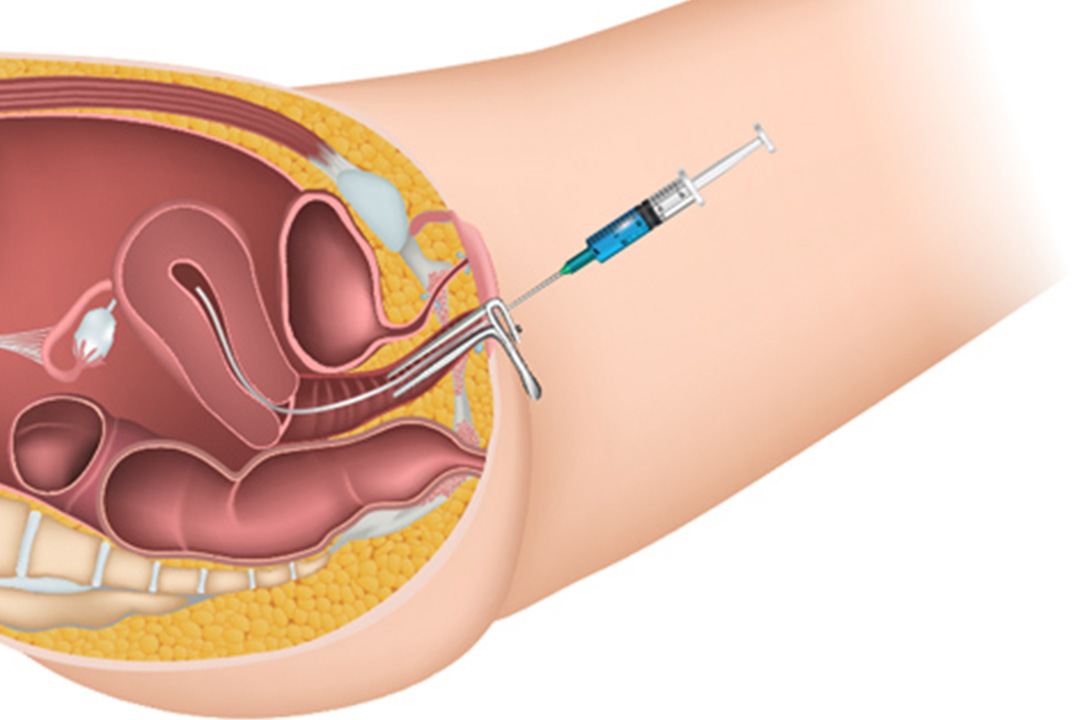
Laparoscopy: Step by Step
Small belly incisions, CO₂ to create space, a camera to see, and instruments to treat.
Under general anesthesia, the abdomen is insufflated with CO₂; a camera is placed through a tiny cut near the navel, and one to two additional small ports are added on the lower abdomen. Dye may be injected through the cervix to check whether the fallopian tubes are open (this is called chromopertubation).
Depending on findings, the team can excise endometriosis, remove ovarian cysts, release adhesions, or perform a myomectomy for select fibroids. You go home the same day in most cases. Shoulder tip pain or bloating over the first 24–48 hours is common from the residual gas.
When to consider Hysteroscopy?
Common indications to choose hysteroscopy involve:
- Irregular or heavy bleeding
- Suspected intracavitary fibroids
- Polyps on ultrasound
- A uterine septum
- Adhesions (Asherman syndrome)
- Retained products
- Recurrent miscarriage
In infertility work-ups, it helps confirm the cavity is normal before embryo transfer or controlled ovarian stimulation. Office hysteroscopy is increasingly used for diagnosis and minor treatment.
When to consider Laparoscopy?
Common indications to choose laparoscopy involve:
- Endometriosis
- Pelvic adhesions
- Ovarian cysts
- Blocked or damaged fallopian tubes
- Fibroids growing on the outer or middle layers of the uterus.
It is also used to evaluate chronic pelvic pain or to manage ectopic pregnancy. In infertility, laparoscopy is often considered after basic testing of both partners, especially if symptoms suggest endometriosis or if imaging suggests tubal disease.
Hysteroscopy and Laparoscopy as Treatment Options
Hysteroscopy (operative): polypectomy, resection of small intracavitary fibroids, lysis of intrauterine adhesions, septum resection, and removal of foreign bodies. Treating these can improve bleeding symptoms and, in selected infertility cases, may improve implantation rates by restoring a normal cavity.
Laparoscopy (operative): excision/ablation of endometriosis, adhesiolysis, ovarian cystectomy, myomectomy (selected cases), salpingostomy/salpingectomy, and tubal neostomy or fimbrioplasty in specific scenarios. These treatments can relieve pain and may improve fertility depending on severity and overall clinical picture.
Safety and Risks
Hysteroscopy: Overall risk is low. Potential complications include uterine perforation, bleeding, infection, and (rarely) problems from the distension fluid such as fluid overload or electrolyte imbalance. Prompt recognition and management keep serious events rare.
Laparoscopy: Risks include injury to bowel, bladder, or blood vessels (most often during entry or trocar placement), bleeding, infection, and anesthesia-related issues. These complications are uncommon in experienced hands, but patients should know the signs that need urgent review after discharge.
Recovery and Downtime
After hysteroscopy, plan for light activity the same day. Cramping and mild spotting may last 24–48 hours. Most people return to work the next day. Your team will advise about when to resume sex or swimming and whether to use pads rather than tampons for a short period.
After laparoscopy, expect bloating or shoulder tip pain for a day or two from the CO₂, plus tenderness at the tiny incisions. Gentle walking helps the gas dissipate. Many people resume desk work in 2–5 days, heavier activity in 1–2 weeks depending on what was done.
How Doctors Choose Between Laparoscopy and Hysteroscopy
If imaging or symptoms point to a cavity problem (like a polyp causing bleeding or a suspected septum in recurrent miscarriage), hysteroscopy is the direct route.
If the clues suggest pelvic disease outside the cavity (pain with periods and intercourse, endometriosis suspicion, cysts, or tube damage), laparoscopy answers more questions and allows broader treatment.
Sometimes both are done in one session: laparoscopy to treat pelvic disease and hysteroscopy to correct a cavity issue, limiting you to one anesthesia event. Your clinician will weigh benefits, recovery time, and fertility plans to tailor the choice.
Special Situations
Planning pregnancy or fertility treatmentA normal uterine cavity is essential for implantation, so hysteroscopy is often used to remove cavity-distorting polyps or fibroids before ovulation induction, IUI, or embryo transfer. Laparoscopy may be offered when endometriosis or tubal pathology is suspected and the results would change the fertility plan.
During pregnancyHysteroscopy is generally avoided in pregnancy unless there is a compelling reason. If a pregnant patient needs abdominal surgery for non-gynecologic reasons (e.g., appendicitis), laparoscopy can be performed safely by experienced teams with adjusted techniques and pressures.
Frequently Asked Questions
Do I need both laparoscopy and hysteroscopy?
Sometimes. If you have symptoms of endometriosis and ultrasound shows a cavity polyp, your team may recommend laparoscopy and hysteroscopy in one sitting so diagnosis and treatment happen together.
Will either laparoscopy and hysteroscopy improve my chances of pregnancy?
It depends on the cause. Removing a cavity-distorting polyp or septum (hysteroscopy) can help implantation. Treating endometriosis or adhesions (laparoscopy) may help some patients, especially when disease is moderate and other factors are favorable. Your overall fertility plan matters as much as the procedure.
Which one hurts more: Laparoscopy and hysteroscopy?
Most diagnostic hysteroscopies are well tolerated with local measures or light sedation; cramping is common but short-lived. Laparoscopy uses general anesthesia, so you don’t feel the surgery itself, but you may feel bloated and sore for a few days afterward.
How long should I take off work after Laparoscopy and hysteroscopy?
After hysteroscopy, many people return the next day. After laparoscopy, 2–5 days is typical for desk jobs, longer if extensive surgery was done. Follow your surgeon’s advice.
What are the red-flag complications I should watch for at home?
Call your team if you develop fever, worsening abdominal pain, heavy bleeding, foul-smelling discharge, fainting, or persistent vomiting. These signs are uncommon but deserve prompt review after any procedure. (This advice aligns with standard post-procedure guidance.)
Conclusion
Hysteroscopy and laparoscopy are complementary tools and not competitors. Hysteroscopy looks inside the uterus and is ideal for diagnosing and correcting cavity problems that can cause bleeding, miscarriages, or implantation failure. Laparoscopy surveys the whole pelvis and treats conditions like endometriosis, adhesions, fibroids on the outside of the uterus, and tubal disease.
The “right” procedure is the one that targets your suspected problem with the least risk and the greatest chance of improving symptoms or fertility. When in doubt, ask your care team what question the procedure is meant to answer and how the result will change your plan.
About Us
AKsigen IVF is a premier center for advanced fertility treatments, with renowned fertility experts on our team. Specializing in IVF, ICSI, egg freezing, and other cutting-edge reproductive technologies, AKsigen IVF is committed to helping couples achieve their dream of parenthood. With personalized care and a patient-first approach, AKsigen IVF provides comprehensive fertility solutions under one roof.