
There is more to the menstrual cycle than simply a monthly event. It is the result of a carefully coordinated sequence of hormonal shifts that prepare the body for pregnancy. Many women track their cycle for a number of reasons, including family planning, symptom management, improving athletic performance or learning more about fertility.
The luteal and follicular phases are two of this cycle's most crucial components. Every stage has a distinct function, hormonal trend, physical symptoms and clinical significance.
If you understand the differences between these two stages, it will help you identify what is normal for your body and when you might require medical care. Couples attempting to conceive, women with irregular cycles and those suffering from premenstrual symptoms or infertility can all benefit from it.
This article will examine both stages in depth, compare their functions and go over possible courses of action in the event that something goes wrong.
What Is the Follicular Phase?
The follicular phase is the first half of the menstrual cycle, beginning on the first day of your period and ending at ovulation.
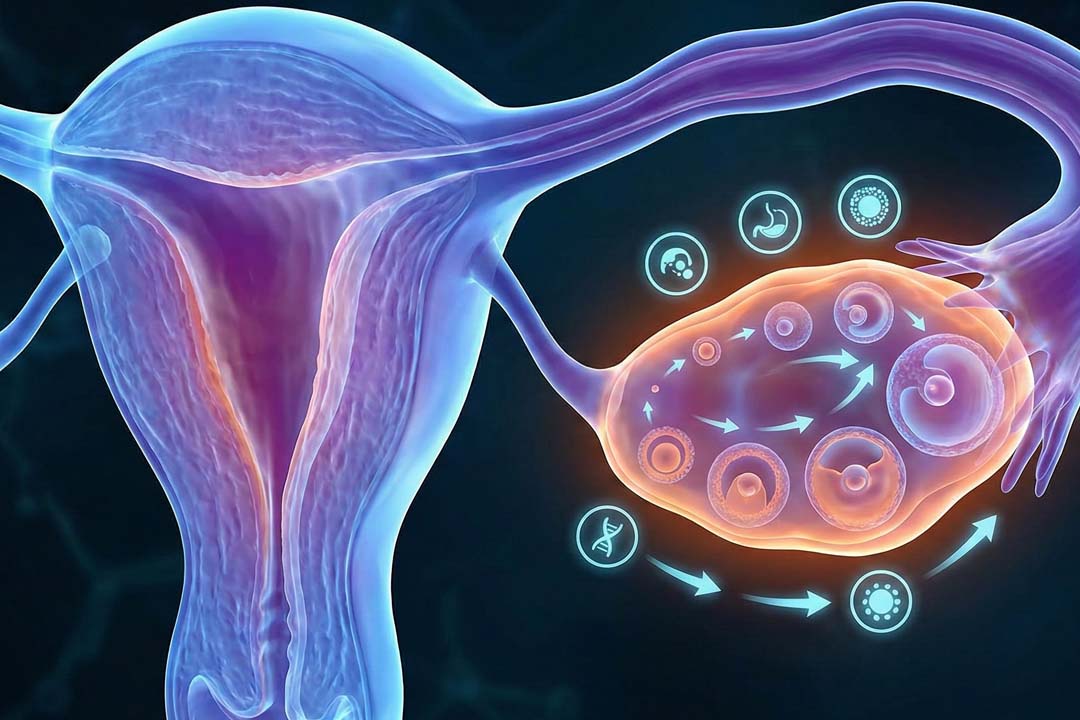
During this phase, the body prepares an egg for release. The brain signals the ovaries through hormones, especially follicle-stimulating hormone or FSH. This hormone stimulates several tiny sacs in the ovary called follicles. Each follicle contains an immature egg. Usually, one follicle becomes dominant and continues to mature.
As the follicle grows, it produces estrogen. Rising estrogen levels thicken the lining of the uterus, known as the endometrium. This lining prepares the uterus for possible implantation of a fertilized egg.
Hormonal Changes in the Follicular Phase
- FSH increases to stimulate egg development
- Estrogen gradually rises
- Luteinizing hormone or LH remains low until just before ovulation
Estrogen also improves cervical mucus quality, making it clearer and more stretchable. This helps sperm travel more easily.
How Long Does the Follicular Phase Last?
The follicular phase can vary in length. In a typical 28 day cycle, it lasts about 14 days. However, it may range from 10 to 16 days in healthy women. This phase is the most flexible part of the cycle and accounts for differences in overall cycle length.
What Is the Luteal Phase?
The luteal phase is the second half of the menstrual cycle, starting after ovulation and ending when the next period begins.
After the egg is released from the ovary, the empty follicle transforms into a structure called the corpus luteum. This structure produces progesterone, the main hormone of the luteal phase.
Progesterone stabilizes and thickens the uterine lining. If pregnancy occurs, progesterone supports early development. If fertilization does not happen, progesterone levels fall. This drop triggers the shedding of the uterine lining, which causes menstruation.
Hormonal Changes in the Luteal Phase
- Progesterone rises sharply
- Estrogen remains present but lower than in the follicular peak
- FSH and LH stay low
Progesterone also raises basal body temperature slightly. Many women track this temperature change to confirm ovulation.
How Long Does the Luteal Phase Last?
The luteal phase is more consistent than the follicular phase. It usually lasts 12 to 14 days. A luteal phase shorter than 10 days may affect fertility and is sometimes referred to as luteal phase defect.
Key Differences Between the Follicular and Luteal Phases
Let us look at the contrast between these two phases and clarify many cycle-related symptoms.
| Feature | Follicular Phase | Luteal Phase |
|---|---|---|
| Timing | Day 1 of period to ovulation | Ovulation to next period |
| Key Hormone | Estrogen | Progesterone |
| Purpose | Egg development | Support potential pregnancy |
| Cervical Mucus | Thin and stretchy | Thick and sticky |
| Body Temperature | Lower | Slightly higher |
| Emotional Pattern | Often more energetic | May feel calm or irritable |
Why Do Symptoms Change Between Phases?
Symptoms change because estrogen and progesterone influence many systems in the body.
Estrogen tends to boost energy, mood, and mental clarity. Many women feel more confident and social during the late follicular phase. Skin may look clearer and workouts may feel easier.
Progesterone, dominant in the luteal phase, has a calming effect but may also cause fatigue, bloating, breast tenderness, and mood shifts. Some women experience premenstrual syndrome or PMS during this time.
Hormonal sensitivity varies. Two women may have very different experiences even if their hormone levels are normal.
Can Irregularities in These Phases Affect Fertility?
Abnormalities in either phase can impact fertility. This is because the events leading up to ovulation and beyond require proper balance between the hormones. If there is any irregularity or imbalance, it will directly impact the entire body physiology.
If the follicular phase is too short or long, ovulation may not occur properly. Without ovulation, pregnancy cannot happen. Conditions such as polycystic ovarian syndrome or thyroid disorders often affect this phase.
If the luteal phase is too short, the uterine lining may not stay stable long enough for implantation. This may lead to difficulty conceiving or early pregnancy loss.
Doctors often evaluate cycle length, ovulation timing, hormone levels, and ultrasound findings when assessing fertility.
Common Problems in the Follicular Phase
Some examples of hormonal irregularities in follicular phase include:
1. Anovulation: This means the ovary does not release an egg. It may cause irregular or missed periods.
2. Poor Follicle Development: Sometimes follicles do not mature properly, leading to low estrogen production.
3. Hormonal Imbalance: High prolactin, thyroid disorders, or stress can disrupt FSH and LH signals.
Common Problems in the Luteal Phase
Some examples of hormonal irregularities in luteal phase include:
1. Luteal Phase Defect: This occurs when progesterone levels are insufficient or the luteal phase is too short.
2. Premenstrual Syndrome: Symptoms include mood swings, bloating, headaches, and food cravings.
3. Severe PMS or PMDD: Premenstrual dysphoric disorder causes intense emotional symptoms that interfere with daily life.
Treatment Options for Follicular Phase Issues
Treatment depends on the underlying cause. Some examples of treatment strategies include:
- Ovulation Induction: Doctors may prescribe medications such as clomiphene citrate or letrozole to stimulate ovulation. These medicines help the body produce and release a mature egg.
- Lifestyle Changes: Maintaining a healthy weight, managing stress, and improving sleep can restore hormonal balance. Even moderate weight loss in overweight women can improve ovulation.
- Thyroid or Hormonal Treatment: If thyroid imbalance or elevated prolactin levels are present, correcting them often normalizes the cycle.
- Assisted Reproductive Techniques: If ovulation does not respond to medication, treatments like intrauterine insemination or IVF may be considered. IVF cost in India generally ranges from INR 1,20,000 to INR 2,50,000 per cycle, depending on medications and procedures required.
Treating underlying conditions
Treatment options for Luteal Phase Defect (LPD) focus on improving progesterone levels and follicle development to support the uterine lining for pregnancy. Key treatments include:
- Medical Treatments: Progesterone Supplementation is often considered the primary treatment, this makes up for insufficient progesterone produced by the corpus luteum. It is administered via vaginal gels/suppositories (highly effective), oral tablets or intramuscular injections.
- Ovulation Induction: Medications are used to stimulate the development of a better-quality follicle, which subsequently produces a stronger corpus luteum.
- hCG Injections: Human Chorionic Gonadotropin (hCG) can be used to stimulate the corpus luteum to produce more of its own progesterone, though it is less common due to the risk of ovarian hyperstimulation syndrome (OHSS)
- SSRIs: For mental health-related luteal phase issues (e.g., PMDD), selective serotonin reuptake inhibitors may be used.
Managing PMS Symptoms
Lifestyle changes help many women. Regular exercise, balanced meals, reducing caffeine, and adequate sleep can ease symptoms. Doctors may recommend:
- Vitamin B6 or magnesium supplements
- Hormonal contraceptives
- Antidepressants for severe Premenstrual Dysphoric Disorder (PMDD)
- Fertility Treatment
If luteal phase defect contributes to infertility, ovulation induction combined with progesterone support may improve implantation chances.
How Do Doctors Evaluate These Phases?
Doctors use several tools to assess cycle health, for instance:
- Blood tests to measure FSH, LH, estrogen, and progesterone
- Ultrasound to track follicle growth and ovulation
- Basal body temperature tracking
- Cycle history analysis
For fertility cases, doctors may also evaluate sperm quality and fallopian tube health.
When Should You See a Doctor?
You should consult a doctor if:
- Periods are consistently irregular
- Cycles are shorter than 21 days or longer than 35 days
- You experience severe PMS symptoms
- You have been trying to conceive for one year without success or six months if over 35
- You notice repeated early pregnancy loss
Can You Support Both Phases Naturally?
Yes, many women benefit from simple lifestyle adjustments for an overall better health and cycle regularity. These include:
- Balanced Nutrition: Include whole grains, protein, fruits, vegetables, and healthy fats. Iron-rich foods support menstrual health.
- Regular Exercise: Moderate physical activity improves insulin sensitivity and hormone balance.
- Stress Management: Chronic stress affects ovulation. Yoga, meditation, and deep breathing exercises help regulate cortisol levels.
- Adequate Sleep: Aim for seven to eight hours of quality sleep daily. Sleep influences reproductive hormones.
Frequently Asked Questions
The follicular phase prepares the egg for release and is estrogen dominant. The luteal phase supports possible pregnancy and is progesterone dominant.
A healthy luteal phase usually lasts 12 to 14 days. A phase shorter than 10 days may affect fertility.
Yes, stress can interfere with hormone signals from the brain, which may delay or prevent ovulation.
IVF cost in India typically ranges from INR 1,20,000 to INR 2,50,000 per cycle, depending on medication, laboratory, and clinical factors.
Low progesterone or a short luteal phase may increase the risk of early pregnancy loss in some women.
No, some women have mild symptoms while others experience more noticeable emotional or physical changes.
Conclusion
Two key parts of the menstrual cycle are the luteal and follicular phases. Each has a unique function in getting the body ready for pregnancy. The cycle runs smoothly when hormones work together harmoniously. The imbalances might lead to symptoms or problems with fertility.
If you understand about these stages, it helps you better understand your body. The first step toward better reproductive health is awareness, whether you are managing PMS, planning a pregnancy or tracking ovulation. Seek early medical attention if you observe problematic symptoms or abnormal patterns. The majority of cycle-related problems can be successfully handled with the right diagnosis and care.
About Us
AKsigen IVF is a premier center for advanced fertility treatments, with renowned fertility experts on our team. Specializing in IVF, ICSI, egg freezing, and other cutting-edge reproductive technologies, AKsigen IVF is committed to helping couples achieve their dream of parenthood. With personalized care and a patient-first approach, AKsigen IVF provides comprehensive fertility solutions under one roof.




 +91 86556 78747
+91 86556 78747 info@aksigenivf.com
info@aksigenivf.com